You might also like
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chinese Oils, Liniments, & PatchesDocument7 pagesChinese Oils, Liniments, & Patchesotro.correo8567No ratings yet
- AKI and CKD MD1TALKDocument14 pagesAKI and CKD MD1TALKAmalNo ratings yet
- Checklist For Cardiopulmonary ResuscitationDocument2 pagesChecklist For Cardiopulmonary Resuscitationvishnu100% (1)
- Thanatology: in All AspectsDocument113 pagesThanatology: in All AspectsVasantha PhutaneNo ratings yet
- FDA Stability Practices For INDDocument28 pagesFDA Stability Practices For INDJumpLinNo ratings yet
- Assignment 7 2overcrowding ED - Edited.editedDocument41 pagesAssignment 7 2overcrowding ED - Edited.editedLetisha PooranNo ratings yet
- Health 6 Curriculum Map 1ST QuarterDocument3 pagesHealth 6 Curriculum Map 1ST QuarterMary Chriszle DomisiwNo ratings yet
- Analogue-Based Drug Discovery: Edited by Jdnos Fischer and C. Robin GanellinDocument12 pagesAnalogue-Based Drug Discovery: Edited by Jdnos Fischer and C. Robin GanellinronyNo ratings yet
- Interpretation: L55 - PSC Jayanagar Home Visit Municipal New No.42, Old No 825, Ground, W K P Road, 7Th Block, JayanagarDocument2 pagesInterpretation: L55 - PSC Jayanagar Home Visit Municipal New No.42, Old No 825, Ground, W K P Road, 7Th Block, JayanagardrmohangNo ratings yet
- Exchange TransfusionDocument13 pagesExchange TransfusionSaba WaheedNo ratings yet
- Stoma Care AlginateDocument6 pagesStoma Care AlginateWiwit ClimberNo ratings yet
- Dengue RDT Laboratory Request FormDocument1 pageDengue RDT Laboratory Request FormJosanne Wadwadan De CastroNo ratings yet
- Lecture Title: Acute Pain Management: Lecturer NameDocument51 pagesLecture Title: Acute Pain Management: Lecturer NameIndra KusumaNo ratings yet
- Ver Berg 2005Document13 pagesVer Berg 2005dio_tansil1317No ratings yet
- Evaluation of Tablet PDFDocument2 pagesEvaluation of Tablet PDFKim50% (2)
- Historical OVERVIEW On Blood BankingDocument4 pagesHistorical OVERVIEW On Blood BankingSogan, MaureenNo ratings yet
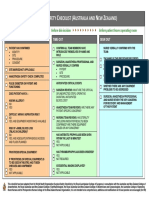
- LST 2009 Surgical Safety Check List (Australia and New Zealand) PDFDocument1 pageLST 2009 Surgical Safety Check List (Australia and New Zealand) PDFaskjhwiuehNo ratings yet
- Perioperative Nursing CareDocument17 pagesPerioperative Nursing CareMisikir Eyob100% (1)
- Shine ClinicDocument6 pagesShine Clinichalasa bethapudiNo ratings yet
- No. 3 - NCM 109LDocument44 pagesNo. 3 - NCM 109LDalene EvangelioNo ratings yet
- Business Prospect and ProposalDocument3 pagesBusiness Prospect and ProposalSUBHANKAR GHOSHNo ratings yet
- Physiotherapy Management Plan PDFDocument3 pagesPhysiotherapy Management Plan PDFsunilbijlani100% (3)
- PDF Nutrition CM 3 CU 11 LAB WEEK 13Document6 pagesPDF Nutrition CM 3 CU 11 LAB WEEK 13Chezer KiethNo ratings yet
- Pressure Flow Urodynamic Studies: The Gold Standard For Diagnosing Bladder Outlet ObstructionDocument8 pagesPressure Flow Urodynamic Studies: The Gold Standard For Diagnosing Bladder Outlet ObstructionmarcelloNo ratings yet
- ThymomasDocument6 pagesThymomasAsmara SyedNo ratings yet
- Prolaps UteriDocument7 pagesProlaps Uteridr.raziNo ratings yet
- Araya Mossie Role Clarification Between Behavioral Science StudiesDocument1 pageAraya Mossie Role Clarification Between Behavioral Science Studiesarayamossie92No ratings yet
- PBLDocument22 pagesPBLOmar AhmedNo ratings yet
- Task 1 - Richela LangoyDocument4 pagesTask 1 - Richela LangoyRiri LangoyNo ratings yet
- Sample Section 504 PlanDocument9 pagesSample Section 504 Planapi-214156276No ratings yet