You might also like
- Exs 387 Lab 7Document7 pagesExs 387 Lab 7api-500055972100% (1)
- Fascial Stretch TherapyDocument294 pagesFascial Stretch TherapyDiana Mariș93% (28)
- Ido's Seminar NotesDocument15 pagesIdo's Seminar NotesAndrei FCFNo ratings yet
- Supraspinatus TendinitisDocument7 pagesSupraspinatus Tendinitismilananand100% (1)
- Section 1. Chapter 1 & 2Document47 pagesSection 1. Chapter 1 & 2Abril Acenas83% (6)
- Conservative Management of Costovertebral SubluxationDocument4 pagesConservative Management of Costovertebral SubluxationDr Franklin Shoenholtz100% (3)
- PositionsDocument40 pagesPositionsVladimir MalusevNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Test Bank For Meeting The Physical Therapy Needs of Children 2nd Edition Susan K EffgenDocument10 pagesTest Bank For Meeting The Physical Therapy Needs of Children 2nd Edition Susan K Effgenmonicafarmerbxtaznmodw100% (19)
- Journal 1 1Document23 pagesJournal 1 1Michel Rigaud100% (3)
- Postural Screening Part 1Document3 pagesPostural Screening Part 1SheenaPerlasNo ratings yet
- Musculoskeletal Exam GuideDocument12 pagesMusculoskeletal Exam GuideAngeliki KostakiNo ratings yet
- Hand and FingerDocument5 pagesHand and FingerkiranNo ratings yet
- David Butler Neural Tissue Mobilisation-1Document11 pagesDavid Butler Neural Tissue Mobilisation-1Himani BhondgeNo ratings yet
- Spine Manipulation ManualDocument14 pagesSpine Manipulation ManualLai Kin KwanNo ratings yet
- Tratamiento Secuencial Curtis1983Document5 pagesTratamiento Secuencial Curtis1983yerec51683No ratings yet
- Best Practice Recommendations For Management of Swan Neck Deformity in Rheumatoid ArthritisDocument10 pagesBest Practice Recommendations For Management of Swan Neck Deformity in Rheumatoid ArthritisAirin QueNo ratings yet
- Gonstead Ifec ProneDocument5 pagesGonstead Ifec ProneAurelien BoschatNo ratings yet
- Musculoskeletal Ultrasound Technical GuidelinesDocument43 pagesMusculoskeletal Ultrasound Technical GuidelinesMarco VincentiNo ratings yet
- Part A: Introduction To The Surface Anatomy of The Thoracic SpineDocument11 pagesPart A: Introduction To The Surface Anatomy of The Thoracic SpineHammad -ullahNo ratings yet
- Examine Cervical Spine Range MotionDocument16 pagesExamine Cervical Spine Range MotionlecturioNo ratings yet
- Wrist Pivot Method of TMJ Dislocation ReductionDocument4 pagesWrist Pivot Method of TMJ Dislocation ReductionRomzi HanifNo ratings yet
- Medial Patellofemoral Ligament Reconstruction With Semi 2013 Arthroscopy TecDocument5 pagesMedial Patellofemoral Ligament Reconstruction With Semi 2013 Arthroscopy TecchinthakawijedasaNo ratings yet
- 32hand ExtensorTendonRepair PDFDocument5 pages32hand ExtensorTendonRepair PDFsenthiljayanthiNo ratings yet
- Modul Antebrachi and ElbowDocument8 pagesModul Antebrachi and Elbowmazidah fauziyyah24No ratings yet
- 09 Cervical Spine 2Document12 pages09 Cervical Spine 2楊畯凱No ratings yet
- Mallet Finger Suturing TechniqueDocument5 pagesMallet Finger Suturing TechniqueSivaprasath JaganathanNo ratings yet
- Pre and Post Operative Physiotherapy Management in Tendon Transfer of HandDocument59 pagesPre and Post Operative Physiotherapy Management in Tendon Transfer of HandjothiNo ratings yet
- Musculoskeletal ExamDocument14 pagesMusculoskeletal ExamS.R.G100% (1)
- The Journal of Foot & Ankle SurgeryDocument4 pagesThe Journal of Foot & Ankle SurgeryEma.diazNo ratings yet
- PNF Techniques in The Upper ExtremityDocument27 pagesPNF Techniques in The Upper ExtremitysanalcrazyNo ratings yet
- Motor Exam GuideDocument16 pagesMotor Exam GuideNohemí Gómez ANo ratings yet
- 1 s2.0 S1877056811000818 MainDocument4 pages1 s2.0 S1877056811000818 MainEvans JohnNo ratings yet
- Positional Relerase TechniqueDocument30 pagesPositional Relerase Techniquebdangar677No ratings yet
- 6 Elbow and WristDocument76 pages6 Elbow and Wristalinaziyad3No ratings yet
- Leech Aveng Von Gs 2016Document12 pagesLeech Aveng Von Gs 2016Andrés Urrego NietoNo ratings yet
- J Jhsa 2017 10 014Document5 pagesJ Jhsa 2017 10 014Nicolas AdrianoNo ratings yet
- ANKLEDocument62 pagesANKLEDokdem AjaNo ratings yet
- Dr. Manjunath Rai, Dr. Sneha Ginimav, Dr. Padmaraj Hegde: Ginwalla's Technique RevisitedDocument6 pagesDr. Manjunath Rai, Dr. Sneha Ginimav, Dr. Padmaraj Hegde: Ginwalla's Technique Revisitedabhishekjha0082No ratings yet
- Muscle Deprogramming - An Orthodontist's Perspective: Batra Laxman Ra Angshuman B LlachDocument5 pagesMuscle Deprogramming - An Orthodontist's Perspective: Batra Laxman Ra Angshuman B LlachJulio Cesar AlvearNo ratings yet
- SPLINTS FOR NBCOTDocument29 pagesSPLINTS FOR NBCOTMarina EskandrousNo ratings yet
- The Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsDocument6 pagesThe Use of A Transolecranon Pin in The Treatment of Flexion-Type SCFsBariša KiršnerNo ratings yet
- Anestesia EspinalDocument8 pagesAnestesia EspinalEgly TuarezNo ratings yet
- Examination of The ShoulderDocument33 pagesExamination of The ShoulderAnonymous 9QxPDpNo ratings yet
- Carpal Tunnel SyndromeDocument27 pagesCarpal Tunnel SyndromeSereinNo ratings yet
- Dr. Bramantya SP Ot - Diagnosis and Management in Upper Extremity ProblemDocument3 pagesDr. Bramantya SP Ot - Diagnosis and Management in Upper Extremity ProblemChristian HarnatNo ratings yet
- 9 CMC and MCP MobilzationDocument9 pages9 CMC and MCP MobilzationGautamNo ratings yet
- Hand & WristDocument56 pagesHand & WristAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Rotator Cuff TendynopatyDocument10 pagesRotator Cuff TendynopatyDipo SiahaanNo ratings yet
- Kinesio Taping Modulo 2Document30 pagesKinesio Taping Modulo 2Angel L Reyes CarrilloNo ratings yet
- Guia de Pontos Motores PDFDocument18 pagesGuia de Pontos Motores PDFDaniel Gonçalves SantosNo ratings yet
- Shoulder ExamDocument24 pagesShoulder ExamMuhammad FahmyNo ratings yet
- 1.教案 the Knee Joint Aspiration (Knee)Document8 pages1.教案 the Knee Joint Aspiration (Knee)林宜璇No ratings yet
- Examining the Hand for Deformities and InjuriesDocument5 pagesExamining the Hand for Deformities and InjuriesGurunadh OrthoNo ratings yet
- MRI Shoulder Protocol: Preparation, Positioning and Imaging StepsDocument27 pagesMRI Shoulder Protocol: Preparation, Positioning and Imaging Stepsدخ D5No ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Neuro 1 and 2 LabDocument3 pagesNeuro 1 and 2 LabHardikPatelNo ratings yet
- 2021 - Chronic Isolated Radial Head DislocationDocument9 pages2021 - Chronic Isolated Radial Head Dislocationjuan pablo aguirreNo ratings yet
- Forearm, Wrist & Hand Special TestDocument17 pagesForearm, Wrist & Hand Special TestelinelisaNo ratings yet
- 1756 153545044822 25Document4 pages1756 153545044822 25sonuNo ratings yet
- Transpalatal Distraction in A Patient With A Narrow MaxillaDocument6 pagesTranspalatal Distraction in A Patient With A Narrow MaxillapetreastefanNo ratings yet
- Mulligan Therapy: What Is It and How Does It WorkDocument33 pagesMulligan Therapy: What Is It and How Does It WorkAgus SantosoNo ratings yet
- Cervical RadiculopathyDocument110 pagesCervical RadiculopathyShabana AfzalNo ratings yet
- Cervical and Lumbar RegionDocument7 pagesCervical and Lumbar RegionVanz AlboNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityFrom EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzNo ratings yet
- Local Flaps in Facial Reconstruction: A Defect Based ApproachFrom EverandLocal Flaps in Facial Reconstruction: A Defect Based ApproachNo ratings yet
- The 5-Minute Neurological Exam SimplifiedDocument43 pagesThe 5-Minute Neurological Exam Simplifiedmandeep axonNo ratings yet
- Spinal Cord InjuryDocument32 pagesSpinal Cord InjuryShubham DaheriyaNo ratings yet
- Wolf Motor Function Test (WMFT) Manual: UAB CI Therapy Research GroupDocument31 pagesWolf Motor Function Test (WMFT) Manual: UAB CI Therapy Research GroupNistara Singh ChawlaNo ratings yet
- MP Medical University B.Sc. Nursing 1st Year Result Dec 2021Document26 pagesMP Medical University B.Sc. Nursing 1st Year Result Dec 2021Shubham DaheriyaNo ratings yet
- President's Address: Trick MovementsDocument3 pagesPresident's Address: Trick MovementsDr. Rushikesh K. Joshi100% (1)
- Feudalism in Ancient IndiaDocument2 pagesFeudalism in Ancient IndiaShubham DaheriyaNo ratings yet
- Discretion of The Court Refers To A JudgeDocument3 pagesDiscretion of The Court Refers To A JudgeShubham DaheriyaNo ratings yet
- Muscles Mouth Eyes Humans Pleasure Sociability Happiness Joy Amusement Anxiety GrimaceDocument1 pageMuscles Mouth Eyes Humans Pleasure Sociability Happiness Joy Amusement Anxiety GrimaceShubham DaheriyaNo ratings yet
- Chapter 3 - Fundamentals of Applied KinesiologyDocument60 pagesChapter 3 - Fundamentals of Applied KinesiologySam100% (1)
- Basketball Strength Training General Preparation ExampleDocument12 pagesBasketball Strength Training General Preparation ExampleChandra IrawanNo ratings yet
- Musculoskeletal DisordersDocument37 pagesMusculoskeletal DisordersRoshani sharmaNo ratings yet
- MMT CERVICAL SPINE MUSCLESDocument11 pagesMMT CERVICAL SPINE MUSCLESApoorvNo ratings yet
- WK 3 Chiro TableDocument4 pagesWK 3 Chiro Tableapi-469904011No ratings yet
- Case Presentation - Closed Fracture Radius Ulna PediatricDocument30 pagesCase Presentation - Closed Fracture Radius Ulna PediatriciamboredtiredNo ratings yet
- Mike Durand-WIAA Off-Season Program Design For Peak PerformanceDocument36 pagesMike Durand-WIAA Off-Season Program Design For Peak PerformancembayabaNo ratings yet
- Neck Pain, Cervical Radiculopathy, and Cervical MyelopathyDocument11 pagesNeck Pain, Cervical Radiculopathy, and Cervical MyelopathyAhmad Shakir100% (1)
- Personal Trainer TextDocument97 pagesPersonal Trainer Textwuddafren100% (1)
- HandbikeDocument10 pagesHandbikeLely JuniariNo ratings yet
- Lower LimbDocument53 pagesLower LimbRupesh M DasNo ratings yet
- Pilates For Hyperlordosis PDFDocument14 pagesPilates For Hyperlordosis PDFkingawitkNo ratings yet
- Attilio Sacripanti - Advances in Judo Biomechanics research-VDM Verlag (2010)Document356 pagesAttilio Sacripanti - Advances in Judo Biomechanics research-VDM Verlag (2010)Marcelo Ruggiero Nor100% (1)
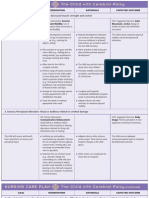
- Nursing Care Plan Goals for Child with Cerebral PalsyDocument3 pagesNursing Care Plan Goals for Child with Cerebral PalsyJamie Icabandi67% (3)
- CMJ Playbook〡Hawkin Dynamics eBook v1Document12 pagesCMJ Playbook〡Hawkin Dynamics eBook v1kzm mzmNo ratings yet
- Block 1 Eccentric Below 80 Triphasic Training Single Legs SpeedDocument2 pagesBlock 1 Eccentric Below 80 Triphasic Training Single Legs SpeedTj NewsomNo ratings yet
- Strength Training For Triathletes Hand OutDocument14 pagesStrength Training For Triathletes Hand OutBrían GohNo ratings yet
- Inmovilizaciones NejmDocument5 pagesInmovilizaciones NejmAndrés PomboNo ratings yet
- Active Elbow, Wrist & Hand Range of MotionDocument3 pagesActive Elbow, Wrist & Hand Range of MotionDee Banayo Bernal PtrpNo ratings yet
- Frozen Shoulder Exercises - tcm28-180808 PDFDocument4 pagesFrozen Shoulder Exercises - tcm28-180808 PDFanalyst_anil14100% (1)
- CNS QuestionsDocument39 pagesCNS QuestionsEvidence ChaibvaNo ratings yet
- FITT 3 REVIEWER DANCE ELEMENTSDocument1 pageFITT 3 REVIEWER DANCE ELEMENTSMicah TaguinodNo ratings yet
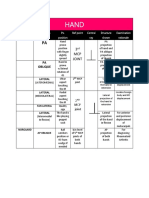
- HAND RadposiDocument1 pageHAND Radposigenel bacaniNo ratings yet