You might also like
- Fifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachFrom EverandFifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachRating: 1 out of 5 stars1/5 (1)
- Studi Kasus Interaksi Obat Case 1Document2 pagesStudi Kasus Interaksi Obat Case 1Amad BelexNo ratings yet
- Remifentanil in The Management of Severe TetanusDocument3 pagesRemifentanil in The Management of Severe TetanusSitiNo ratings yet
- Treatment of Status Migrainosus by General AnestheDocument3 pagesTreatment of Status Migrainosus by General AnesthenurulwindianggrainiNo ratings yet
- 1 s2.0 S0033318220302073 MainDocument4 pages1 s2.0 S0033318220302073 MainAnonymous ZSmSZErTqtNo ratings yet
- Studi Kasus MK Konsep Terapi Genap 2019.2020 - UkbDocument8 pagesStudi Kasus MK Konsep Terapi Genap 2019.2020 - UkbYossi KhrismaeniNo ratings yet
- Idiopathic HiccupDocument3 pagesIdiopathic HiccupSuresh IndiaNo ratings yet
- Citalopram ManiaDocument6 pagesCitalopram Maniagion.nandNo ratings yet
- Menometrorrhagia and Tachyarrhythmia After Using Oral and Topical GinsengDocument4 pagesMenometrorrhagia and Tachyarrhythmia After Using Oral and Topical Ginsengkartika adyaniNo ratings yet
- Kwong YLDocument2 pagesKwong YLpharmaNo ratings yet
- Letters To The Editor: One Personal Copy May Be PrintedDocument3 pagesLetters To The Editor: One Personal Copy May Be PrintedEdo Wahyu PratamaNo ratings yet
- Withdrawal Seizure Associated With High Dosage of Aripiprazole and Fluoxetine: A Case ReportDocument3 pagesWithdrawal Seizure Associated With High Dosage of Aripiprazole and Fluoxetine: A Case ReportwsandoNo ratings yet
- Case Report Hydromorphone Precipitating Serotonin SyndromeDocument4 pagesCase Report Hydromorphone Precipitating Serotonin SyndromeMax PowellsNo ratings yet
- Movement Disord Clin Pract - 2014 - Sprenger - Perimenstrual Fluctuations in Two Siblings With Early Onset Parkinson SDocument3 pagesMovement Disord Clin Pract - 2014 - Sprenger - Perimenstrual Fluctuations in Two Siblings With Early Onset Parkinson Shajjar.rima93No ratings yet
- Walker 1953Document3 pagesWalker 1953Diego SobrevillaNo ratings yet
- Cardiac Arrest Upon Induction of General AnesthesiaDocument7 pagesCardiac Arrest Upon Induction of General AnesthesiaIlona HiariejNo ratings yet
- P ('t':'3', 'I':'3053856877') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document2 pagesP ('t':'3', 'I':'3053856877') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Reza SatriaNo ratings yet
- Venlafaxine and Chronic PainDocument2 pagesVenlafaxine and Chronic PainteddypolNo ratings yet
- Delirium As A Contributing Factor To "Crescendo" Pain: Three Case ReportsDocument4 pagesDelirium As A Contributing Factor To "Crescendo" Pain: Three Case ReportsHenrikNo ratings yet
- Ketamine For Opiate WithdrawalDocument3 pagesKetamine For Opiate WithdrawalroboNo ratings yet
- Patient Case PresentationDocument26 pagesPatient Case PresentationKathleen B BaldadoNo ratings yet
- Hypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaDocument4 pagesHypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaAnnisaa RizqiyanaNo ratings yet
- Convulsions After Enflurane in A Schizophrenic Patient Receiving NeurolepticsDocument3 pagesConvulsions After Enflurane in A Schizophrenic Patient Receiving NeurolepticsJoão VítorNo ratings yet
- Client Care Study of MissDocument32 pagesClient Care Study of MissTolulade OlubenaNo ratings yet
- Olanzapine Induced Hyperprolactinemia: IjbcpDocument2 pagesOlanzapine Induced Hyperprolactinemia: IjbcpIrma SetyawatiNo ratings yet
- AmiodaroneDocument2 pagesAmiodaronematin5No ratings yet
- Tramadol and Bladder DysfunctionDocument2 pagesTramadol and Bladder DysfunctionFred DeeNo ratings yet
- Case Study Guide 2: Awful Pain PillsDocument11 pagesCase Study Guide 2: Awful Pain PillsAila Marie ArandillaNo ratings yet
- 2014 EJA, Ondansetron Oculogyric CrisisDocument2 pages2014 EJA, Ondansetron Oculogyric CrisisAirwayNo ratings yet
- Anesthesia Management in A Patient With Systemic LDocument3 pagesAnesthesia Management in A Patient With Systemic Laieyha hamkaNo ratings yet
- Clozapine Associated DeliriumDocument2 pagesClozapine Associated DeliriumPutu Agus GrantikaNo ratings yet
- 2015 Article 20Document5 pages2015 Article 20anaNo ratings yet
- Discinesia e SNM Litio e Antipsicotico InicioDocument4 pagesDiscinesia e SNM Litio e Antipsicotico InicioBárbara LimaNo ratings yet
- Ispub 11731Document4 pagesIspub 11731Putri YingNo ratings yet
- Schizophrenia TreatmentDocument4 pagesSchizophrenia TreatmentPutra DariusNo ratings yet
- Mignogna Et Al-2002-Journal of Oral Pathology & Medicine PDFDocument7 pagesMignogna Et Al-2002-Journal of Oral Pathology & Medicine PDFdrjonduNo ratings yet
- Diazepam in Severe Tetanus TreatmentDocument6 pagesDiazepam in Severe Tetanus Treatmentselvie87No ratings yet
- 18.jaladi Himaja Battu Rakesh PDFDocument9 pages18.jaladi Himaja Battu Rakesh PDFFebby da costaNo ratings yet
- 23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25Document5 pages23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25observacionfray23No ratings yet
- Intranasal Substituted Cathinone Bath Salts .2Document6 pagesIntranasal Substituted Cathinone Bath Salts .2Mr. FNo ratings yet
- Iadt 07 I 5 P 427Document2 pagesIadt 07 I 5 P 427Fendy PrasetyoNo ratings yet
- Brief Case Reports of Medically Supervised, Water-Only Fasting Associated With Remission of Autoimmune Disease PDFDocument3 pagesBrief Case Reports of Medically Supervised, Water-Only Fasting Associated With Remission of Autoimmune Disease PDFpaulabenderNo ratings yet
- Flumazenil KLSDocument1 pageFlumazenil KLSNiniNo ratings yet
- Prog Neurol Psychiatry - 2022 - Mashimo - Polyarthralgia With Oral RisperidoneDocument2 pagesProg Neurol Psychiatry - 2022 - Mashimo - Polyarthralgia With Oral RisperidoneFachry RahmanNo ratings yet
- Isoniazid Induced AnaphylaxisDocument3 pagesIsoniazid Induced AnaphylaxisLuciana OliveiraNo ratings yet
- Late Postpartum EclampsiaDocument4 pagesLate Postpartum Eclampsiaapi-3702092No ratings yet
- Interaction 1Document4 pagesInteraction 1urdhalokdas2001No ratings yet
- InteractionDocument4 pagesInteractionurdhalokdas2001No ratings yet
- Review Article: Herpes Zoster in Older Adults and Worsening of Life QualityDocument36 pagesReview Article: Herpes Zoster in Older Adults and Worsening of Life QualityAlmiraNurArofahNo ratings yet
- Case 15-2007: A 20-Year-Old Woman With Asthma and Cardiorespiratory ArrestDocument9 pagesCase 15-2007: A 20-Year-Old Woman With Asthma and Cardiorespiratory ArresteliNo ratings yet
- Case Report Skizofrenia KatatonikDocument3 pagesCase Report Skizofrenia KatatonikIntan PratiwiNo ratings yet
- Benzodiazepine Allergy With Anesthesia Administration: A Review of Current LiteratureDocument8 pagesBenzodiazepine Allergy With Anesthesia Administration: A Review of Current LiteratureWahyudi WahyudiNo ratings yet
- Rifampicin-Induced Fever: L P Meena, M Rai, A Pathak, Sunny Garg, Anju BhartiDocument2 pagesRifampicin-Induced Fever: L P Meena, M Rai, A Pathak, Sunny Garg, Anju BhartiInternational Organization of Scientific Research (IOSR)No ratings yet
- 10 Infectious DiseaseDocument42 pages10 Infectious Diseaseandirio7486No ratings yet
- Case Presentation 2Document11 pagesCase Presentation 2Angel Jonele ManongsongNo ratings yet
- Prurigo NodularisDocument5 pagesPrurigo NodularisRobith LubisNo ratings yet
- Case Report AsliDocument4 pagesCase Report AsliLidiaNo ratings yet
- The Effects of Laparoscopic Nissen FundoplicationDocument2 pagesThe Effects of Laparoscopic Nissen FundoplicationGabriel CassNo ratings yet
- Chinese HerbDocument3 pagesChinese HerbwengweiNo ratings yet
- Selected Topics: Toxicology: Severe Carisoprodol Withdrawal After A 14-Year Addiction and Acute OverdoseDocument4 pagesSelected Topics: Toxicology: Severe Carisoprodol Withdrawal After A 14-Year Addiction and Acute OverdoseAhmad SyaukatNo ratings yet
- JCM 10 04900Document14 pagesJCM 10 04900Chistian LassoNo ratings yet
- 2020 Annual Report of The American Association of Poison Control Centers National Poison Data System NPDS 38th Annual ReportDocument221 pages2020 Annual Report of The American Association of Poison Control Centers National Poison Data System NPDS 38th Annual ReportChistian LassoNo ratings yet
- Sulfasalazine Toxic Reactions. Hepatitis, Fever, and Skin Rash With Hypocomplementemia and Immune ComplexesDocument2 pagesSulfasalazine Toxic Reactions. Hepatitis, Fever, and Skin Rash With Hypocomplementemia and Immune ComplexesChistian LassoNo ratings yet
- Sulphasalazine Induced DRESSDocument3 pagesSulphasalazine Induced DRESSChistian LassoNo ratings yet
- Rash and Fever After Sulfasalazine UseDocument5 pagesRash and Fever After Sulfasalazine UseChistian LassoNo ratings yet
- Sulfasalazine Induced DRESS Syndrome A Review of Case ReportsDocument11 pagesSulfasalazine Induced DRESS Syndrome A Review of Case ReportsChistian LassoNo ratings yet
- DRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisDocument4 pagesDRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisChistian LassoNo ratings yet
- Rifamycins and Anti-Diabetic Agents Drug-Drug InteractionsDocument2 pagesRifamycins and Anti-Diabetic Agents Drug-Drug InteractionsmoniaNo ratings yet
- Atosiban-5ml InfusionDocument5 pagesAtosiban-5ml InfusionMd. Abdur RahmanNo ratings yet
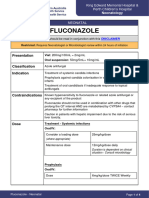
- FluconazoleDocument4 pagesFluconazoleeucaNo ratings yet
- Psychopharmacology Article StyleDocument9 pagesPsychopharmacology Article StyleLizethNo ratings yet
- Summary Barang Masuk Dan Keluar: Nama Item Kategori Item Kode ItemDocument96 pagesSummary Barang Masuk Dan Keluar: Nama Item Kategori Item Kode ItemTitha RahmiNo ratings yet
- Detail Sertifikat TKDN Obat ObatanDocument116 pagesDetail Sertifikat TKDN Obat Obatannakes puskesmas Kecamatan Cempaka PutihNo ratings yet
- Mapeh 6 Health PPT q4 - MedicinesDocument17 pagesMapeh 6 Health PPT q4 - MedicinesMaureen VillacobaNo ratings yet
- Inevntory With ExpDocument64 pagesInevntory With ExpDin DinNo ratings yet
- Rekapitulasi Februari 2023Document13 pagesRekapitulasi Februari 2023hanafiNo ratings yet
- OB Doctors Orders (Answer Key)Document3 pagesOB Doctors Orders (Answer Key)Ryan-Jay AbolenciaNo ratings yet
- HJM 25 Okt 2023Document16 pagesHJM 25 Okt 2023Mel WsNo ratings yet
- Biperiden Baseline AssessmentDocument2 pagesBiperiden Baseline AssessmentKasandra Dawn BerisoNo ratings yet
- Detil Barang Bpba Yang Sudah Maduk Dan Belum MasukDocument5 pagesDetil Barang Bpba Yang Sudah Maduk Dan Belum Masukbrilyant phascoNo ratings yet
- Group 5 Pdis211 Lab E1Document22 pagesGroup 5 Pdis211 Lab E1Mikaela Kean JoseNo ratings yet
- DRUGDocument13 pagesDRUGReniNo ratings yet
- Farsk Health - Order Sheet 2023Document1 pageFarsk Health - Order Sheet 2023nazila.mazhari08No ratings yet
- Beginners Guide To DigitalRXDocument14 pagesBeginners Guide To DigitalRXStarrx714No ratings yet
- Pharmaceutical Calculations 13th - Ansel-1-1Document2 pagesPharmaceutical Calculations 13th - Ansel-1-1فاطمة عدنان حسينNo ratings yet
- Pharmanovaprice List July ExcelDocument13 pagesPharmanovaprice List July ExcelSagar GargNo ratings yet
- The Prevention & Treatment of Augmentation: Mark J Buchfuhrer, MDDocument22 pagesThe Prevention & Treatment of Augmentation: Mark J Buchfuhrer, MDdo leeNo ratings yet
- Order CITO 11.07.2022Document6 pagesOrder CITO 11.07.2022lintiaNo ratings yet
- Antipsychotics,-WPS OfficeDocument7 pagesAntipsychotics,-WPS Officermconvidhya sri2015No ratings yet
- Comparing Generic and Innovator Drugs A Review ofDocument16 pagesComparing Generic and Innovator Drugs A Review ofPrachi PandeyNo ratings yet
- GENERAL ANAESTHESIA - Presentation Editted RecordedDocument31 pagesGENERAL ANAESTHESIA - Presentation Editted RecordedTatenda SibandaNo ratings yet
- Blood Giving Set Versus Infusion (Iv Giving) SetDocument3 pagesBlood Giving Set Versus Infusion (Iv Giving) SetTiktok- AfricaNo ratings yet
- Pre-Registration Completeness Checklist Document For Copy Drug, Jul-2012Document5 pagesPre-Registration Completeness Checklist Document For Copy Drug, Jul-2012adite_alifaNo ratings yet
- Opiods MorphineDocument4 pagesOpiods MorphinevysakhmohanannairNo ratings yet
- How The Body Affects The Drugs: College of Health SciencesDocument42 pagesHow The Body Affects The Drugs: College of Health SciencesNat Lynne Distor TrondilloNo ratings yet
- SPH Untuk Rsud BKKMDocument57 pagesSPH Untuk Rsud BKKMBagas PutranandaNo ratings yet
- Veterinary Pharmacology and Toxicology MCQsDocument18 pagesVeterinary Pharmacology and Toxicology MCQsSunil97% (63)