You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- BSBINN601Document42 pagesBSBINN601Joanne Navarro Almeria78% (23)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 12 Rights of Safe Drug AdministrationDocument2 pages12 Rights of Safe Drug Administrationlilcheeza77% (74)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nosotros NoDocument2 pagesNosotros NoAlcindorLeadonNo ratings yet
- Essentials of Community Medicine - A Practical Approach PDFDocument487 pagesEssentials of Community Medicine - A Practical Approach PDFamarhadid70% (20)
- A Six Step Approach To Writing A Formal SummaryDocument5 pagesA Six Step Approach To Writing A Formal SummaryБезымянный КактусNo ratings yet
- ML SyllDocument2 pagesML Syllmurlak37No ratings yet
- Managing Corporate Real Estate: Leading and Emerging PracticesDocument24 pagesManaging Corporate Real Estate: Leading and Emerging PracticesramyeidNo ratings yet
- FMU 101 - Chap 4 - Test Taking Strategies Part IIDocument11 pagesFMU 101 - Chap 4 - Test Taking Strategies Part IIMario LaraNo ratings yet
- Smart GoalsDocument3 pagesSmart Goalsapi-290230693No ratings yet
- Underground Interrogation With Steve CotterDocument12 pagesUnderground Interrogation With Steve CotterTom HillNo ratings yet
- Combined Science: Trilogy: 8464/B/1F - Biology Paper 1 Foundation Tier Mark SchemeDocument22 pagesCombined Science: Trilogy: 8464/B/1F - Biology Paper 1 Foundation Tier Mark SchemeLabeenaNo ratings yet
- TVEC Guide to Sri Lanka's Vocational Education SystemDocument31 pagesTVEC Guide to Sri Lanka's Vocational Education Systemshishir_cNo ratings yet
- Digital Citizenship vs. Global CitizenshipDocument20 pagesDigital Citizenship vs. Global CitizenshipMacasinag Jamie Anne M.No ratings yet
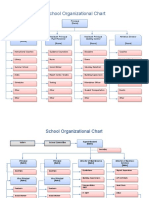
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- Risk ManagementDocument15 pagesRisk ManagementABEGAIL MADLAONo ratings yet
- k5 - Sistem Informasi KesehatanDocument29 pagesk5 - Sistem Informasi KesehatanannisaNo ratings yet
- Audiometer Impedqnce Audiometer AT235 - USER - MANUALDocument103 pagesAudiometer Impedqnce Audiometer AT235 - USER - MANUALKafina Multi SejahteraNo ratings yet
- mgmt404 Final Project HMPDocument22 pagesmgmt404 Final Project HMPapi-25526962850% (2)
- Principles of Monitoring & Evaluation - NotesDocument113 pagesPrinciples of Monitoring & Evaluation - NotesKeith100% (2)
- Oral Surgery Maxill - Anesthesia TechniquesDocument4 pagesOral Surgery Maxill - Anesthesia TechniquesSaif AyedNo ratings yet
- PSYCHOLOGY Lesson 2Document15 pagesPSYCHOLOGY Lesson 2KOSTKANo ratings yet
- Job Responsibilities PresentationDocument14 pagesJob Responsibilities PresentationFiftys Sabz KedewaNo ratings yet
- ReportingDocument4 pagesReportingMark CalimlimNo ratings yet
- Curriculum Vitae: Amir E. Ibrahim, M.DDocument11 pagesCurriculum Vitae: Amir E. Ibrahim, M.DkendoNo ratings yet
- COMPENSATION Class 1 PDFDocument5 pagesCOMPENSATION Class 1 PDFpsicologothNo ratings yet
- CBSE Class 6 Science Components of Food MCQs Set A, Multiple Choice Questions For ScienceDocument4 pagesCBSE Class 6 Science Components of Food MCQs Set A, Multiple Choice Questions For ScienceNinaNo ratings yet
- Hts Policy PhilippinesDocument15 pagesHts Policy PhilippinesBrunxAlabastro100% (1)
- Prolonged Fasting - How Is It PosiblerDocument17 pagesProlonged Fasting - How Is It PosiblersaturninojonesNo ratings yet
- Writing Sample 2Document9 pagesWriting Sample 2api-582848179No ratings yet
- Veterinarians 03-2023Document13 pagesVeterinarians 03-2023PRC BaguioNo ratings yet