You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cabin Crew Recruitment - Pre Employment Medical Check Form.Document3 pagesCabin Crew Recruitment - Pre Employment Medical Check Form.Vigor DjuricNo ratings yet
- Epidemiologi Manajerial: Oleh: Ubaidillah S.Si.,M.Kes, EpidDocument26 pagesEpidemiologi Manajerial: Oleh: Ubaidillah S.Si.,M.Kes, Epidhesty marliaNo ratings yet
- Shot Put Official NotesDocument6 pagesShot Put Official NotesJyotirmayeeNo ratings yet
- Neurodevelopmental Outcomes of Preterm Infants: A Recent Literature ReviewDocument6 pagesNeurodevelopmental Outcomes of Preterm Infants: A Recent Literature ReviewJyotirmayeeNo ratings yet
- Semister QuestionDocument1 pageSemister QuestionJyotirmayeeNo ratings yet
- Management PancreaticDocument10 pagesManagement PancreaticJyotirmayeeNo ratings yet
- Clinical Manifestation of Necrotizing EnterocolitiDocument6 pagesClinical Manifestation of Necrotizing EnterocolitiJyotirmayeeNo ratings yet
- PSM QuestionsDocument4 pagesPSM QuestionsJyotirmayeeNo ratings yet
- Somnath HoreDocument61 pagesSomnath HoreJyotirmayeeNo ratings yet
- Ent History Taking and Examination-1Document16 pagesEnt History Taking and Examination-1Jyotirmayee100% (5)
- PSM 2020-2008 Regular Question Papers WBUHS © Medical JunctionDocument15 pagesPSM 2020-2008 Regular Question Papers WBUHS © Medical JunctionJyotirmayeeNo ratings yet
- Modified Valsalva Manoeuvre For Supraventricular TachycardiaDocument3 pagesModified Valsalva Manoeuvre For Supraventricular TachycardiaJyotirmayeeNo ratings yet
- Ultrastructure of Epidermolysis V. Epidermolysis Simplex LocalisataDocument5 pagesUltrastructure of Epidermolysis V. Epidermolysis Simplex LocalisataJyotirmayeeNo ratings yet
- BurnsDocument25 pagesBurnsJyotirmayeeNo ratings yet
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- Admission Admtsston: Murmu &Document13 pagesAdmission Admtsston: Murmu &JyotirmayeeNo ratings yet
- Ra 7600 PDFDocument5 pagesRa 7600 PDFanorith88No ratings yet
- Evaluacion Ingles Constanza Jarpa Aedo 7mo Basico UlaDocument4 pagesEvaluacion Ingles Constanza Jarpa Aedo 7mo Basico UlaCaterine Aedo BerrocalNo ratings yet
- Free Download PDF DeVita, Hellman, and Rosenberg's Cancer Principles & Practice of OncologyDocument100 pagesFree Download PDF DeVita, Hellman, and Rosenberg's Cancer Principles & Practice of OncologyZhou RuojingNo ratings yet
- HA-RLE-WS # 3 Assessing Mental Status and Substance AbuseDocument7 pagesHA-RLE-WS # 3 Assessing Mental Status and Substance AbuseJULIE ANNE CORTEZNo ratings yet
- The History of MicrobiologyDocument3 pagesThe History of MicrobiologyAsfi Raian OmeNo ratings yet
- AbortionDocument5 pagesAbortionYlenol HolmesNo ratings yet
- Final Scientific Program EORCAPS 2013 For StudentsDocument3 pagesFinal Scientific Program EORCAPS 2013 For StudentsdrgauravkguptaNo ratings yet
- FIA Meter: Fluorescence Immunoassay Rapid Quantitative TestDocument2 pagesFIA Meter: Fluorescence Immunoassay Rapid Quantitative TestJM Umayam100% (1)
- Staphylococcosis Infection in ChickensDocument6 pagesStaphylococcosis Infection in ChickensShah NawazNo ratings yet
- BlepharitisDocument4 pagesBlepharitisnan623No ratings yet
- New - PPT - VINAYAKDocument123 pagesNew - PPT - VINAYAKAnimesh AryaNo ratings yet
- Jurnal 2 - PICO and Critical AppraisalDocument3 pagesJurnal 2 - PICO and Critical AppraisalRezki Pratama SadeliNo ratings yet
- Thromboangiitis ObliteransDocument17 pagesThromboangiitis Obliteransmu_crNo ratings yet
- Marketing Plan Sensodyne ToothpasteDocument22 pagesMarketing Plan Sensodyne ToothpasteMd. Azad HossainNo ratings yet
- Question NEURODocument39 pagesQuestion NEUROjondelacruz19100% (1)
- New Drug Application HardDocument37 pagesNew Drug Application HardGANESH KUMAR JELLA100% (1)
- Weber's TestDocument9 pagesWeber's Testapi-3769252100% (2)
- Mtwo NiTi Rotary SystemDocument10 pagesMtwo NiTi Rotary SystemVioleta BotnariNo ratings yet
- Jurnal MaternitasDocument11 pagesJurnal MaternitasEndyNo ratings yet
- 07 Pediatrics in Review July20Document65 pages07 Pediatrics in Review July20AlmaNo ratings yet
- PPT-"D-Cycloserine: A Novel Treatment For Gulf War Illness" - Dr. Rosemary ToomeyDocument9 pagesPPT-"D-Cycloserine: A Novel Treatment For Gulf War Illness" - Dr. Rosemary ToomeyAnthony HardieNo ratings yet
- Nurse Resident Resume Dayna ValdezDocument2 pagesNurse Resident Resume Dayna Valdezapi-304925106No ratings yet
- SCHIZODocument25 pagesSCHIZOQuinonez Anna MarieNo ratings yet
- DEVELOPING PHYSIOTHERAPY LED SHOULDER CLINICS: A PROPOSAL TO ADJUST SCOPE OF PRACTICE BY TENDAYI MUTSOPOTSI Bsc. HPT (Hons) MSc. ORTHO-MEDDocument15 pagesDEVELOPING PHYSIOTHERAPY LED SHOULDER CLINICS: A PROPOSAL TO ADJUST SCOPE OF PRACTICE BY TENDAYI MUTSOPOTSI Bsc. HPT (Hons) MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- Polycystic Ovary Syndrome (PCOS) : February 2020Document5 pagesPolycystic Ovary Syndrome (PCOS) : February 2020Lia MeivianeNo ratings yet
- Case Study, Chapter 20, Assessment of Respiratory FunctionDocument11 pagesCase Study, Chapter 20, Assessment of Respiratory FunctionMaddyNo ratings yet
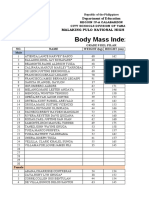
- Bmi FinalDocument38 pagesBmi FinalWalden Dela PenaNo ratings yet
- Rational Drug Use (Rdu) - Clin Pharma - IDocument3 pagesRational Drug Use (Rdu) - Clin Pharma - IKandysse de OcampoNo ratings yet