You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Alert Level 2 Guidelines From DOH and IATFDocument4 pagesAlert Level 2 Guidelines From DOH and IATFJenny Vi de CastroNo ratings yet
- 1 SMDocument14 pages1 SMRatnaNo ratings yet
- Olympic DHBB - Anh 11 - Chuyên Biên Hòa - Hà NamDocument16 pagesOlympic DHBB - Anh 11 - Chuyên Biên Hòa - Hà NamVy PhạmNo ratings yet
- Ebook Foundations For Population Health in Community Public Health Nursing PDF Full Chapter PDFDocument67 pagesEbook Foundations For Population Health in Community Public Health Nursing PDF Full Chapter PDFmargaret.forbes670100% (21)
- Sars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRDocument3 pagesSars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRAmbareen AbidNo ratings yet
- Reading and Writing SkillsDocument6 pagesReading and Writing SkillsAngela UntalanNo ratings yet
- RA For Smart LockerDocument2 pagesRA For Smart LockerSuresh NaiduNo ratings yet
- 12.07.2021 GHMC SPL Drive Session Sites.Document3 pages12.07.2021 GHMC SPL Drive Session Sites.Rohit VemulaNo ratings yet
- Ciad 696Document10 pagesCiad 696vsjsqz97nrNo ratings yet
- Digital COVID Certificate Certificat Digital CovidDocument2 pagesDigital COVID Certificate Certificat Digital CovidНадежда ФаинаNo ratings yet
- 26-01-2022 HMB EnglishDocument84 pages26-01-2022 HMB EnglishNarasimha KulkarniNo ratings yet
- Nejmoa 2301425Document12 pagesNejmoa 2301425carb0ne14rNo ratings yet
- Philippine Airlines-Travel GuidelinesDocument7 pagesPhilippine Airlines-Travel GuidelinesJOCELYN TEJADANo ratings yet
- Plate01 - Fidel, Jared Hope G (General Hospital)Document86 pagesPlate01 - Fidel, Jared Hope G (General Hospital)Charles Dominic Reyes TapnioNo ratings yet
- WHO PHL COVID 19 Situation Report 114Document9 pagesWHO PHL COVID 19 Situation Report 114jessica sugaboNo ratings yet
- TAFFIX SCIENCE PAPER Feb 2021Document10 pagesTAFFIX SCIENCE PAPER Feb 2021Sanja IlićNo ratings yet
- HG5 - Covid-19 PathologyDocument9 pagesHG5 - Covid-19 PathologySulaesih AQNo ratings yet
- EAPP Module Week 4Document8 pagesEAPP Module Week 4Aurora FontanillaNo ratings yet
- Wetransfer - ProjectDocument40 pagesWetransfer - ProjectĐinh ThắngNo ratings yet
- Coronavirus Flow Chart Response Plan (Vessel - Site)Document2 pagesCoronavirus Flow Chart Response Plan (Vessel - Site)HSE PULAI ANo ratings yet
- CertificateDocument1 pageCertificateZainab KhanNo ratings yet
- Coronavirus (COVID-19) Records PDFDocument2 pagesCoronavirus (COVID-19) Records PDF35130030ksrNo ratings yet
- RRL and Question Self Protective BehaviorDocument2 pagesRRL and Question Self Protective BehaviorMaica LectanaNo ratings yet
- Yazan Nedal Jamil Aldeen - F - 19092022215830Document1 pageYazan Nedal Jamil Aldeen - F - 19092022215830Yazan JamalaldeenNo ratings yet
- MutationDocument6 pagesMutationALEJANDRO COUTIÑO VALDOVINOSNo ratings yet
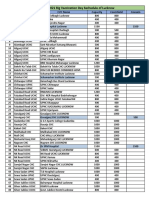
- 27th Sep 2021 Big Vaccination Day Sechedule of LucknowDocument9 pages27th Sep 2021 Big Vaccination Day Sechedule of LucknowAmit YadavNo ratings yet
- The Weakening of The Economy in Indonesia During The Corona Virus Disease-19 Pandemic: The Tourism SectorDocument10 pagesThe Weakening of The Economy in Indonesia During The Corona Virus Disease-19 Pandemic: The Tourism SectorYossy Eka PraditaNo ratings yet
- Welcome Back To Shaklee Shops: Fun Dip Special!Document1 pageWelcome Back To Shaklee Shops: Fun Dip Special!asmawi bin hashimNo ratings yet
- Ischemic Stroke in COVID-19-Positive Patients - An Overview of SARS-CoV-2 and Thrombotic Mechanisms For The NeurointerventionalistDocument6 pagesIschemic Stroke in COVID-19-Positive Patients - An Overview of SARS-CoV-2 and Thrombotic Mechanisms For The Neurointerventionalistarif 2006No ratings yet
- Nasal Spray (1222)Document11 pagesNasal Spray (1222)Kapital SenturiNo ratings yet