You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Gamak MotorDocument34 pagesGamak MotorCengiz Sezer100% (1)
- 12.5 Collision Theory - ChemistryDocument15 pages12.5 Collision Theory - ChemistryAri CleciusNo ratings yet
- Dawn of Solar PV CookingDocument5 pagesDawn of Solar PV CookingAbhinav AgrawalNo ratings yet
- Purpose in LifeDocument1 pagePurpose in Lifeaashish95100% (1)
- Biophoton RevolutionDocument3 pagesBiophoton RevolutionVyavasayaha Anita BusicNo ratings yet
- IMO Ship Waste Delivery Receipt Mepc - Circ - 645Document1 pageIMO Ship Waste Delivery Receipt Mepc - Circ - 645wisnukerNo ratings yet
- 3D Proportional Condylectomy 1Document4 pages3D Proportional Condylectomy 1tamisatnamNo ratings yet
- Semi Automated Three Dimensional Condylar Reconstruction.Document5 pagesSemi Automated Three Dimensional Condylar Reconstruction.tamisatnamNo ratings yet
- Mandibular Reconstruction With Tissue EngineeringDocument5 pagesMandibular Reconstruction With Tissue EngineeringtamisatnamNo ratings yet
- Airway Volume Changes After Orthognathic Surgery in Patients With Down SyndromeDocument14 pagesAirway Volume Changes After Orthognathic Surgery in Patients With Down SyndrometamisatnamNo ratings yet
- Effect of Mono and BimaxillaryDocument6 pagesEffect of Mono and BimaxillarytamisatnamNo ratings yet
- Column, Slab, Footing and Wall Footing Foundations: Class A MixingDocument47 pagesColumn, Slab, Footing and Wall Footing Foundations: Class A MixingGioharry Nul PanambulanNo ratings yet
- Semi Finals in Tle 2015Document3 pagesSemi Finals in Tle 2015LoraineTenorioNo ratings yet
- Crouse Hinds XPL Led BrochureDocument12 pagesCrouse Hinds XPL Led BrochureBrayan Galaz BelmarNo ratings yet
- Physical and Morphological Characterisation of Typha Australis FibresDocument12 pagesPhysical and Morphological Characterisation of Typha Australis FibresIJAR JOURNALNo ratings yet
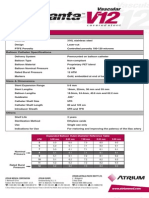
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- A Year On A FarmDocument368 pagesA Year On A FarmvehapkolaNo ratings yet
- Assessment Questions: 1: Wash - Rinse and SanitizeDocument3 pagesAssessment Questions: 1: Wash - Rinse and SanitizeAna Margarita AycochoNo ratings yet
- G1CDocument12 pagesG1CKhriz Ann C ÜNo ratings yet
- Sat Vocabulary Lesson and Practice Lesson 5Document3 pagesSat Vocabulary Lesson and Practice Lesson 5api-430952728No ratings yet
- Comparing Exponential NumbersDocument5 pagesComparing Exponential NumbersMaya RahayuNo ratings yet
- GP1 Q1 Week-1Document18 pagesGP1 Q1 Week-1kickyknacksNo ratings yet
- PIX4D Simply PowerfulDocument43 pagesPIX4D Simply PowerfulJUAN BAQUERONo ratings yet
- Passenger Lift Alert - Health and Safety AuthorityDocument4 pagesPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiNo ratings yet
- Parts Catalogue of Foton: (TC2A504-034K)Document132 pagesParts Catalogue of Foton: (TC2A504-034K)МаксимNo ratings yet
- Cost Analysis - Giberson Art GlassDocument3 pagesCost Analysis - Giberson Art GlassSessy Saly50% (2)
- Biomedical Engineering Handbook Revised 5 2015Document37 pagesBiomedical Engineering Handbook Revised 5 2015Teja GuttiNo ratings yet
- RACI Matrix Design For Managing Stakeholders in PRDocument12 pagesRACI Matrix Design For Managing Stakeholders in PRRheza Nugraha Prabareswara100% (1)
- Esteem 1999 2000 1.3L 1.6LDocument45 pagesEsteem 1999 2000 1.3L 1.6LArnold Hernández CarvajalNo ratings yet
- 9 5 - 358 362 PDFDocument5 pages9 5 - 358 362 PDFمالك مناصرةNo ratings yet
- 07ercoskun 05 01 PDFDocument23 pages07ercoskun 05 01 PDFjagmadridNo ratings yet
- 12/1/2014 Powder MetallurgyDocument29 pages12/1/2014 Powder Metallurgysofyan sam0% (2)
- Someone Who Believes in YouDocument1 pageSomeone Who Believes in YouMANOLO C. LUCENECIONo ratings yet
- Rekomendasi AnimeDocument11 pagesRekomendasi Animeosvaldo manurungNo ratings yet
- SambongDocument3 pagesSambongNica Del GallegoNo ratings yet