You might also like
- Working Memory and Auditory Processing in School-Age ChildrenDocument15 pagesWorking Memory and Auditory Processing in School-Age ChildrenvviraaNo ratings yet
- 2014mshahandouts StoeckelDocument37 pages2014mshahandouts StoeckelAna Vogeley100% (1)
- A at Motor SpeechDocument5 pagesA at Motor SpeechNini JohannaNo ratings yet
- PmvbedsideevaluationDocument2 pagesPmvbedsideevaluationapi-114739487No ratings yet
- Pediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDocument6 pagesPediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDiego Vargas LópezNo ratings yet
- Motor Speech Skills in Down SyndromeDocument11 pagesMotor Speech Skills in Down SyndromePaulaNo ratings yet
- Aphasia TableDocument2 pagesAphasia TableFajar Rudy QimindraNo ratings yet
- Icd 10 Codes SLPDocument79 pagesIcd 10 Codes SLPvviraa100% (2)
- Aphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpDocument4 pagesAphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpTarienNo ratings yet
- Dysarthria ChartDocument12 pagesDysarthria ChartTalia Garcia100% (1)
- Mount Wilga Hight Level Language TestDocument78 pagesMount Wilga Hight Level Language TestbonnieNo ratings yet
- Aphasia: Hana Nabila Ulfia 1102014118Document14 pagesAphasia: Hana Nabila Ulfia 1102014118hana nabilaNo ratings yet
- Apraxia TXDocument20 pagesApraxia TXadriricaldeNo ratings yet
- Admission:Discharge Criteria in Speech-Language Pathology - ASHADocument16 pagesAdmission:Discharge Criteria in Speech-Language Pathology - ASHANádia MarquesNo ratings yet
- Aphasia 07Document34 pagesAphasia 07razik89No ratings yet
- Hyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- How - . - I Train Others in Dysphagia.Document5 pagesHow - . - I Train Others in Dysphagia.Speech & Language Therapy in PracticeNo ratings yet
- Clinical Review: Dysarthria, HypokineticDocument19 pagesClinical Review: Dysarthria, HypokineticRashid HussainNo ratings yet
- Classification of Velopharyngeal DysfunctionDocument1 pageClassification of Velopharyngeal DysfunctionVictoria Rojas AlvearNo ratings yet
- Swallow Screening ToolDocument1 pageSwallow Screening Toolidris Lajide100% (1)
- Acquired Apraxia of Speech Treatment Overview PDFDocument12 pagesAcquired Apraxia of Speech Treatment Overview PDFHaroun Krilov-Egbert100% (1)
- Shipping Point DeterminationDocument10 pagesShipping Point DeterminationAnupa Wijesinghe80% (5)
- Early Echoic Skills Assessment (EESA) : Barbara E. Esch, PH.D., BCBA, CCC-SLPDocument4 pagesEarly Echoic Skills Assessment (EESA) : Barbara E. Esch, PH.D., BCBA, CCC-SLPvviraa0% (4)
- Post Stroke WritingDocument9 pagesPost Stroke WritingAdi ParamarthaNo ratings yet
- Articulation and Phonological Processess SummarisedDocument2 pagesArticulation and Phonological Processess SummarisedSuné GreeffNo ratings yet
- TRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNDocument50 pagesTRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHN100% (5)
- Ccu PSG en DysphagiaDocument52 pagesCcu PSG en DysphagiaTni JolieNo ratings yet
- Nkosi Sharpe Assessment MSD 08Document9 pagesNkosi Sharpe Assessment MSD 08Paula QuezadaNo ratings yet
- Contributions of Morphological Awareness Skills To Word-Level Reading and Spelling in First-Grade Children With and Without Speech Sound DisorderDocument17 pagesContributions of Morphological Awareness Skills To Word-Level Reading and Spelling in First-Grade Children With and Without Speech Sound DisordervviraaNo ratings yet
- APPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJODocument150 pagesAPPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (2)
- Treatment of Oropharyngeal Dysphagia CarolMcKee (1) DPNS StudyDocument23 pagesTreatment of Oropharyngeal Dysphagia CarolMcKee (1) DPNS Studyconstantineelia100% (1)
- Oral Sensorimotor Therapy in Pediatric DysphagiaDocument1 pageOral Sensorimotor Therapy in Pediatric Dysphagiashaghala38No ratings yet
- Communication Disorders Quarterly 2010 Bahr 131 8Document9 pagesCommunication Disorders Quarterly 2010 Bahr 131 8LauraLunguNo ratings yet
- Joseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)Document531 pagesJoseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)szeho chanNo ratings yet
- Effectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisDocument54 pagesEffectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisconstantineeliaNo ratings yet
- Evaluating and Treating Communication and Cognitive Disorders - Approaches To Referral and Collaboration For Speech-Language Pathology and Clinical NeuropsychologyDocument16 pagesEvaluating and Treating Communication and Cognitive Disorders - Approaches To Referral and Collaboration For Speech-Language Pathology and Clinical Neuropsychologyluribe662No ratings yet
- Phacodynamics: Phacoemulsification For Residents Unpad - Cicendo Eye Hospital 2020Document40 pagesPhacodynamics: Phacoemulsification For Residents Unpad - Cicendo Eye Hospital 2020GabrielaNo ratings yet
- Western Aphasia Battery Revised Pearson Clinical NaDocument4 pagesWestern Aphasia Battery Revised Pearson Clinical NaBryan Kagz0% (1)
- Diseases of Esophagus.Document3 pagesDiseases of Esophagus.Isabel Castillo100% (2)
- Guss DisfagiaDocument4 pagesGuss DisfagiaNinoska OrtizNo ratings yet
- Dysphagia & Related Disorder ManagementDocument12 pagesDysphagia & Related Disorder ManagementVedashri14100% (1)
- Videofluoroscopic Swallowing StudiesDocument25 pagesVideofluoroscopic Swallowing StudiesPriisciilla Vicencio100% (1)
- Jim DX Report RedactedDocument3 pagesJim DX Report Redactedapi-543869960No ratings yet
- Entrepreneurship LAS Lesson-1 Week1Document7 pagesEntrepreneurship LAS Lesson-1 Week1Shanna kaye rallosNo ratings yet
- NursingBedsideSwallowingScreen PDFDocument1 pageNursingBedsideSwallowingScreen PDFLUCASNo ratings yet
- Medical Examination Form - Juvenile: Part 1: Statement To The Medical ExaminerDocument4 pagesMedical Examination Form - Juvenile: Part 1: Statement To The Medical ExaminerMohd Rafie HashimNo ratings yet
- Fois ScaleDocument1 pageFois Scalemaria.castillo1047897No ratings yet
- Dysphagia ManagementDocument10 pagesDysphagia ManagementTempleknight7No ratings yet
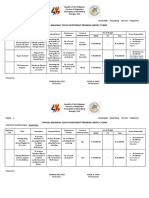
- Annual Barangay Youth Investment Program (Abyip) Cy 2020Document6 pagesAnnual Barangay Youth Investment Program (Abyip) Cy 2020Michael Louie Iglesias100% (3)
- A Comparison of Two Treatments For Childhood Apraxia of Speech - Methods and Treatment Protocol For A Parallel Group Randomised Control TrialDocument9 pagesA Comparison of Two Treatments For Childhood Apraxia of Speech - Methods and Treatment Protocol For A Parallel Group Randomised Control TrialCamila CruzNo ratings yet
- Aws Final ReportDocument27 pagesAws Final Reportkiswah computers100% (2)
- Natalie Brickner-Slp ResumeDocument1 pageNatalie Brickner-Slp Resumeapi-238387904No ratings yet
- Assessment and Treatment of Linguistic Deficits PDFDocument96 pagesAssessment and Treatment of Linguistic Deficits PDFJumraini TammasseNo ratings yet
- CEcover904 p2Document4 pagesCEcover904 p2Antonio MezzopreteNo ratings yet
- Fluoroscopic Evaluation of Oropharyngeal Dysphagia - Anatomic, Technical, and Common Etiologic Factors - ManuscritoDocument25 pagesFluoroscopic Evaluation of Oropharyngeal Dysphagia - Anatomic, Technical, and Common Etiologic Factors - ManuscritoandrefaelNo ratings yet
- DLP Science 3Document148 pagesDLP Science 3hasnifa100% (27)
- Dysphagia AssessmentDocument2 pagesDysphagia AssessmentTRUE FAITH YUQUIMPONo ratings yet
- Dysphagia Handicap Index (DHI) : Please Place A Check in The Box That Describes Your Swallowing DifficultyDocument2 pagesDysphagia Handicap Index (DHI) : Please Place A Check in The Box That Describes Your Swallowing DifficultyAylin Sanhueza Toledo67% (3)
- 2016 Duffy JR - Motor Speech Disorders Where Will We BeDocument6 pages2016 Duffy JR - Motor Speech Disorders Where Will We BeCarol TibaduizaNo ratings yet
- VitalStim Electrode Placement GuideDocument1 pageVitalStim Electrode Placement GuideMd Sherajul HaqueNo ratings yet
- Ico Oscar SicsDocument5 pagesIco Oscar Sicsbrahmani pitanatriNo ratings yet
- Habla ClaraDocument14 pagesHabla ClaraCristóbal Landeros TorresNo ratings yet
- ORLADocument10 pagesORLACarol CoelhoNo ratings yet
- Dysphagia NotesDocument5 pagesDysphagia Notesapi-31372205650% (2)
- AphasiaDocument8 pagesAphasiaapi-308647214No ratings yet
- Blue Dye TestDocument9 pagesBlue Dye TestMacarena Elizabeth Olavarría Gómez100% (1)
- Cilt HandoutDocument4 pagesCilt Handoutapi-454269640No ratings yet
- Treatment of Wernicke'S Aphasia With Jargon: A Case StudyDocument11 pagesTreatment of Wernicke'S Aphasia With Jargon: A Case StudyIvanaNo ratings yet
- Prevention Program BrochureDocument2 pagesPrevention Program Brochureapi-232834696No ratings yet
- Speech and Language: Advances in Basic Research and PracticeFrom EverandSpeech and Language: Advances in Basic Research and PracticeNo ratings yet
- Clinical Immunology Nima Rezaei Full ChapterDocument51 pagesClinical Immunology Nima Rezaei Full Chaptertim.morrison630100% (15)
- Blue and White Simple Technology Keynote PresentationDocument15 pagesBlue and White Simple Technology Keynote PresentationPsicología ULS 2018No ratings yet
- Compare Apple Ipad Pro 12.9 (2018) vs. Apple Ipad Pro 12.9 (2020) vs. Apple Ipad Pro 12.9 (2021)Document3 pagesCompare Apple Ipad Pro 12.9 (2018) vs. Apple Ipad Pro 12.9 (2020) vs. Apple Ipad Pro 12.9 (2021)dacrysNo ratings yet
- Evidence of Cycles in European Commercial Real Estate Markets - and Some HypothesesDocument18 pagesEvidence of Cycles in European Commercial Real Estate Markets - and Some HypothesesMaryna BolotskaNo ratings yet
- Data Wrangling and AnalysisDocument36 pagesData Wrangling and AnalysisAshish Antopazhunkaran100% (1)
- 2-French Colonial ArchitectureDocument71 pages2-French Colonial ArchitectureGlory Chhajed67% (3)
- DrowningDocument9 pagesDrowningCarlos Alberto Torres LópezNo ratings yet
- Ventilation GuidlineDocument17 pagesVentilation GuidlineJatuporn Boontang100% (1)
- Eaton 9SX UPS: High Performance Online Double Conversion UPSDocument2 pagesEaton 9SX UPS: High Performance Online Double Conversion UPScesar1023No ratings yet
- Mysteries of The Holy RosaryDocument3 pagesMysteries of The Holy RosaryTimothy Justin FranciscoNo ratings yet
- Assessment Task Document of Instructions BDocument8 pagesAssessment Task Document of Instructions Bapi-327869042No ratings yet
- EThics WrittenDocument16 pagesEThics WrittenVinod Thomas EfiNo ratings yet
- Heating Baking Drying CookingDocument4 pagesHeating Baking Drying CookingPrashant RohillaNo ratings yet
- Introduction To ZariDocument10 pagesIntroduction To Zarijanhavi madaanNo ratings yet
- Aws 517Document22 pagesAws 517afarmaiaNo ratings yet
- Configuring Your Computer and Network Adapters For Best Performance Application NoteDocument13 pagesConfiguring Your Computer and Network Adapters For Best Performance Application NotekeoxxNo ratings yet
- Rodrigo Zhang: English As A Second LanguageDocument1 pageRodrigo Zhang: English As A Second LanguageRodrigo ZhangNo ratings yet
- MisoprostolDocument2 pagesMisoprostolDr-Jagadeesh MangamooriNo ratings yet
- Design, Analysis and Optimization of Six Cylinders Compressed Air Radial EngineDocument8 pagesDesign, Analysis and Optimization of Six Cylinders Compressed Air Radial EngineAbhishek MeNo ratings yet
- Republic Act 10533 - JeanDocument2 pagesRepublic Act 10533 - JeanJean AmbrocioNo ratings yet
- 01-01 Introduction To BSCDocument6 pages01-01 Introduction To BSCAwa StelkNo ratings yet