You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
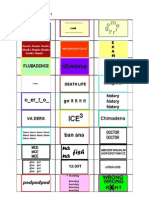
- Rebus Puzzles & KeyDocument4 pagesRebus Puzzles & KeyWilliam C F ChongNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Helping Brands Tap Into Vietnams Changing Eating Habits PDFDocument68 pagesHelping Brands Tap Into Vietnams Changing Eating Habits PDFHoang Nguyen MinhNo ratings yet
- HEALTH 7 EXAM (2nd Quarter) QuestionsDocument4 pagesHEALTH 7 EXAM (2nd Quarter) QuestionsKert Cyrel RomeroNo ratings yet
- SB Resolution Adoption of eOPT 2012Document3 pagesSB Resolution Adoption of eOPT 2012Babuu BabuuNo ratings yet
- Dr. Joel WallachDocument10 pagesDr. Joel WallachfabriciopNo ratings yet
- Hibiscus Rosa-SinensisDocument32 pagesHibiscus Rosa-SinensisShanthi_KVNo ratings yet
- Turnip: A Nutrient Capsule For The People of LadakhDocument2 pagesTurnip: A Nutrient Capsule For The People of Ladakhanwar hussainNo ratings yet
- 2022 FM3 SEND Week 2Document11 pages2022 FM3 SEND Week 2jedisavage MinecraftNo ratings yet
- Smoothie DietDocument7 pagesSmoothie DietMiriam Mantolan100% (1)
- Jurnal Penggunaan Waktu Ekstraksi Berbeda Terhadap Aktivitas Antioksidan TERIPANG KELING (Holothuria Atra)Document11 pagesJurnal Penggunaan Waktu Ekstraksi Berbeda Terhadap Aktivitas Antioksidan TERIPANG KELING (Holothuria Atra)Fitri WijayaNo ratings yet
- Diabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Document19 pagesDiabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Karen Kate AblesNo ratings yet
- Case 39-2020: A 29-Month-Old Boy With Seizure and HypocalcemiaDocument10 pagesCase 39-2020: A 29-Month-Old Boy With Seizure and HypocalcemiaGeneNo ratings yet
- Katindig, Mary Joy, A.Document2 pagesKatindig, Mary Joy, A.katindigmjNo ratings yet
- Abstract of Price QuotationDocument3 pagesAbstract of Price QuotationKingman AbdulganiNo ratings yet
- Infant FeedingDocument26 pagesInfant Feedingabdelrahmanmoselhy122No ratings yet
- The Role of Lifestyle in Male Infertility: Diet, Physical Activity, and Body HabitusDocument10 pagesThe Role of Lifestyle in Male Infertility: Diet, Physical Activity, and Body HabitusSantiago CeliNo ratings yet
- Old-Fashioned Potato Soup RecipeDocument1 pageOld-Fashioned Potato Soup RecipearkcaverNo ratings yet
- DSWD: Policies and Programs That Impact EducationDocument2 pagesDSWD: Policies and Programs That Impact EducationShaNe BesaresNo ratings yet
- Red Mango PDFDocument47 pagesRed Mango PDFIsniharah PangandamanNo ratings yet
- UNIT Meal Planning and PreparationDocument25 pagesUNIT Meal Planning and PreparationFransiska Way Warti RobertsonNo ratings yet
- Lista Suplimentelor Alimentare Notificate 1228 - 2020Document45 pagesLista Suplimentelor Alimentare Notificate 1228 - 2020Krystyan KellerNo ratings yet
- The Calorie: Myth, Measurement, and Reality: American Journal of Clinical Nutrition December 1995Document9 pagesThe Calorie: Myth, Measurement, and Reality: American Journal of Clinical Nutrition December 1995Filip MilicevicNo ratings yet
- LGC AXIO QFCS Web+Application+Form+2023Document16 pagesLGC AXIO QFCS Web+Application+Form+2023ryzki marthaNo ratings yet
- Sourdough Starter GuideDocument8 pagesSourdough Starter GuideSvet HeidiNo ratings yet
- Benefits and UsesDocument7 pagesBenefits and UsesLadylyn BatacNo ratings yet
- Hippo S19 Reading Preliminary 2022Document10 pagesHippo S19 Reading Preliminary 2022adnen ferjaniNo ratings yet
- Soal Pas Bahasa Inggris Kelas 9Document5 pagesSoal Pas Bahasa Inggris Kelas 9엘라이나No ratings yet
- Ajol File Journals - 246 - Articles - 163938 - Submission - Proof - 163938 2929 423769 1 10 20171211Document6 pagesAjol File Journals - 246 - Articles - 163938 - Submission - Proof - 163938 2929 423769 1 10 20171211Rafael Pedro BautistaNo ratings yet
- Nutrelief:: Food Security Nutrition IIRR'sDocument2 pagesNutrelief:: Food Security Nutrition IIRR'sKirstein ItliongNo ratings yet
- Menu Planning Chapter 8Document25 pagesMenu Planning Chapter 8Maou SamaNo ratings yet