You might also like
- # 1 Initial Data BaseDocument6 pages# 1 Initial Data BaseAmor Vince Shantel B.No ratings yet
- Tool FAMILY HEALTH CARE PROCESS 1Document5 pagesTool FAMILY HEALTH CARE PROCESS 1nadzwa velascoNo ratings yet
- Community Survey ToolDocument3 pagesCommunity Survey ToolMARWA MAMONGCAL100% (1)
- Community Health Assessment FormDocument2 pagesCommunity Health Assessment FormMary May Revilla MarceloNo ratings yet
- Family Assessment ToolDocument7 pagesFamily Assessment ToolKing Aldus ConstantinoNo ratings yet
- Community Health Survey FormDocument2 pagesCommunity Health Survey FormArvin Jon Bislig50% (2)
- Oncology Nursing Health AssessmentDocument2 pagesOncology Nursing Health AssessmentkisNo ratings yet
- Appendix C Survey QuestionnaireDocument9 pagesAppendix C Survey QuestionnaireFranz SalazarNo ratings yet
- Pedia HX Profile SheetDocument10 pagesPedia HX Profile SheetMarlon BauagNo ratings yet
- ) Case Study (Document3 pages) Case Study (rudra_mazumdarNo ratings yet
- BioPsychoSocial JongsmaDocument4 pagesBioPsychoSocial Jongsmarredmond100% (1)
- Letter RequestDocument8 pagesLetter RequestShikarin KitaNo ratings yet
- HOUSE HOLD PERFORMA Final (DR - Syma)Document3 pagesHOUSE HOLD PERFORMA Final (DR - Syma)saraNo ratings yet
- Adoption-App 0218 PDFDocument4 pagesAdoption-App 0218 PDFaaaaNo ratings yet
- 7.4 Vulnerable Orphans Children Project Enrollement FormDocument8 pages7.4 Vulnerable Orphans Children Project Enrollement Formمتعلم لغة أنجليزيةNo ratings yet
- Student Health Record PDFDocument2 pagesStudent Health Record PDFailen joy villoNo ratings yet
- DCNHS GF1 Cumulative Folder PDFDocument4 pagesDCNHS GF1 Cumulative Folder PDFPrincess Aurelio50% (2)
- Student Individual Inventory FormDocument2 pagesStudent Individual Inventory Formnatsu dragneel100% (1)
- Form 4b v050120Document4 pagesForm 4b v050120Estarmio ZaficoNo ratings yet
- Eastern Visayas Regional Covid-19 Testing Center: Laboratory Test Request FormDocument1 pageEastern Visayas Regional Covid-19 Testing Center: Laboratory Test Request FormLouieNo ratings yet
- Case Investigation Form: DiphtheriaDocument3 pagesCase Investigation Form: DiphtheriaSalihu MustaphaNo ratings yet
- Medical Record FormDocument3 pagesMedical Record FormBDL SkinNo ratings yet
- CHN Survery FormulationDocument2 pagesCHN Survery FormulationJemima Nove JapitanaNo ratings yet
- Selective Genetic BreedingDocument6 pagesSelective Genetic BreedingDavid OtooNo ratings yet
- CHN Survey FormDocument5 pagesCHN Survey FormPʀɩŋcɘss LɩʌNo ratings yet
- Student HealthDocument2 pagesStudent HealthNathan ChaceNo ratings yet
- CODINGDocument3 pagesCODINGHà NgânNo ratings yet
- CoopMED Health Insurance Doctor Examination FormDocument2 pagesCoopMED Health Insurance Doctor Examination FormKammieNo ratings yet
- Student InventoryDocument2 pagesStudent InventoryMikee SantoNo ratings yet
- CEIR Registration Form FrontDocument2 pagesCEIR Registration Form Frontjhon villafuerteNo ratings yet
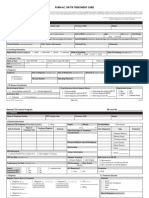
- Individual Treatment Record: Province of Iloilo Municipality of MaasinDocument1 pageIndividual Treatment Record: Province of Iloilo Municipality of MaasinMa. Theresse Vicky A. MatesNo ratings yet
- LS - GCL - Individual Above NEL Form - FillableDocument1 pageLS - GCL - Individual Above NEL Form - FillableJerald Peter VargasNo ratings yet
- Appendices: Saint Mary'S University Bayombong, Nueva Vizcaya School of Health Sciences Community Survey FormDocument13 pagesAppendices: Saint Mary'S University Bayombong, Nueva Vizcaya School of Health Sciences Community Survey FormMartin ManuelNo ratings yet
- Medical Certificate: (To Be Filled-Out by The Applicant)Document3 pagesMedical Certificate: (To Be Filled-Out by The Applicant)Hinata BiancaNo ratings yet
- Form 4c v050120Document8 pagesForm 4c v050120talbaruelNo ratings yet
- Structured Questionaire: Vijay Marie College of Nursing Begumpet, HyderabadDocument16 pagesStructured Questionaire: Vijay Marie College of Nursing Begumpet, Hyderabadkalla sharonNo ratings yet
- CHN Kuesioner 2018 - InggrisDocument7 pagesCHN Kuesioner 2018 - InggrisMuhammad AriefNo ratings yet
- PPBCC: Spay and Neuter Surgery Consent Form: Please Answer The Following Questions BelowDocument2 pagesPPBCC: Spay and Neuter Surgery Consent Form: Please Answer The Following Questions Belowmae cendanaNo ratings yet
- Cor Jesu College, Inc.: Family Health SurveyDocument6 pagesCor Jesu College, Inc.: Family Health Survey2BGrp3Plaza, Anna MaeNo ratings yet
- Community Health Assessment FormDocument4 pagesCommunity Health Assessment Formracel joyce gemotoNo ratings yet
- Questionnaire Nutrition FieldDocument5 pagesQuestionnaire Nutrition FieldNoel KalagilaNo ratings yet
- Family Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingDocument4 pagesFamily Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- Bibliography Books: JournalsDocument6 pagesBibliography Books: JournalsSukruth SNo ratings yet
- Patient Medical HistoryDocument5 pagesPatient Medical HistoryTamara WilliamsonNo ratings yet
- Family Assessment Tool 2022 1Document3 pagesFamily Assessment Tool 2022 1stephanie serdoncilloNo ratings yet
- Barangay Profiling QuestionnaireDocument20 pagesBarangay Profiling QuestionnaireHa MidNo ratings yet
- Initial Data Base QuestionnaireDocument3 pagesInitial Data Base QuestionnaireMariahnaSadjaluddinNo ratings yet
- Alcohol Use Disorders Identification Test (AUDIT)Document2 pagesAlcohol Use Disorders Identification Test (AUDIT)Teresa Meehan100% (2)
- Full Questionnaire Acceptance, Attitudes, and Willingness To Pay For A Future COVID-19 VaccinationDocument5 pagesFull Questionnaire Acceptance, Attitudes, and Willingness To Pay For A Future COVID-19 VaccinationKevin SebastianNo ratings yet
- Questionnaire To Find Demographic and Clinical Characteristics of Patients With Cerebral Palsy at Shaikh Zayed HospitalDocument2 pagesQuestionnaire To Find Demographic and Clinical Characteristics of Patients With Cerebral Palsy at Shaikh Zayed HospitalZenabNaazNo ratings yet
- Tools Section - I Demographic Variables InstructionDocument10 pagesTools Section - I Demographic Variables InstructionRaniNo ratings yet
- 2023 Renal Questionnaire - Asante AKyem North For REDCApDocument7 pages2023 Renal Questionnaire - Asante AKyem North For REDCAposeik1233No ratings yet
- Birth PlanDocument2 pagesBirth PlanAnn Camille RosalesNo ratings yet
- DiseasesDocument3 pagesDiseasesKeith PintoNo ratings yet
- Tool 21 Jan' EngDocument8 pagesTool 21 Jan' Eng19 - Miten KariyaNo ratings yet
- PWD Form PDFDocument1 pagePWD Form PDFAdrian Pastor100% (1)
- First-Time Membership ApplicationDocument1 pageFirst-Time Membership Applicationonect100% (2)
- Salmonella Typhi: Typhoid Fever, Also Known Simply As Typhoid, Is A Bacterial Infection DueDocument1 pageSalmonella Typhi: Typhoid Fever, Also Known Simply As Typhoid, Is A Bacterial Infection DueIna Dwi RahmanikaNo ratings yet
- Case Study Questionnaire For Malnourished ChildrenDocument5 pagesCase Study Questionnaire For Malnourished ChildrenSta Cruz BacnotanNo ratings yet
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDocument19 pagesLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroNo ratings yet
- Ortd 323-Answer Key: Final Examination Thursday, June 13, 2002Document10 pagesOrtd 323-Answer Key: Final Examination Thursday, June 13, 2002Ali AlyaNo ratings yet
- Cataract Classification 2003Document8 pagesCataract Classification 2003Abdelrahman M. AlnweiriNo ratings yet
- Pitfalls of Trauma Care: Dr. Nicole P. Hart Consultant Emergency Physician Associate Lecturer TraumaDocument62 pagesPitfalls of Trauma Care: Dr. Nicole P. Hart Consultant Emergency Physician Associate Lecturer TraumaGiovanni HenryNo ratings yet
- Fake Abortion Form TemplateDocument4 pagesFake Abortion Form Templateyouismyfavcolour67% (3)
- Herpes Zoster!Document26 pagesHerpes Zoster!Ruth Faustine Jontah Rayo100% (1)
- Iteration 1: Decomposition (How Would You Break Down Your Problem Into Sub-Problems?Document10 pagesIteration 1: Decomposition (How Would You Break Down Your Problem Into Sub-Problems?Pandu HutagalungNo ratings yet
- WHO Operational Handbook On Tuberculosis 2020Document136 pagesWHO Operational Handbook On Tuberculosis 2020Hanifah HanifahNo ratings yet
- Account Sales Manager Biotechnology Pharmaceutical in Phoenix AZ Resume Walter NedzaDocument2 pagesAccount Sales Manager Biotechnology Pharmaceutical in Phoenix AZ Resume Walter NedzaWalterNedzaNo ratings yet
- MCQs in PediatricsDocument4 pagesMCQs in Pediatricsarun babu93% (15)
- EAACI Guideline: Anaphylaxis (2021 Update) : GuidelinesDocument21 pagesEAACI Guideline: Anaphylaxis (2021 Update) : GuidelinesYuly GómezNo ratings yet
- Polo Labs, IVY Hospital, Sector Polo Labs, IVY Hospital, Sector-71, MohaliDocument1 pagePolo Labs, IVY Hospital, Sector Polo Labs, IVY Hospital, Sector-71, MohaliRaman ChandiNo ratings yet
- Pediatric Critical Care Medicine: EditorsDocument269 pagesPediatric Critical Care Medicine: EditorsCk1NhiKhoa2020 chuyenkhoaNo ratings yet
- Instructor Guide For Introduction To TCCC-MP 180801Document16 pagesInstructor Guide For Introduction To TCCC-MP 180801M. Owen ErwinNo ratings yet
- Family & Home NursingDocument77 pagesFamily & Home NursingNancy SinghNo ratings yet
- 2023 - Registration FormDocument3 pages2023 - Registration FormhusnanabiyyuNo ratings yet
- Intl J Gynecology Obste - 2020 - Killeen - Examining The Use of The FIGO Nutrition Checklist in Routine AntenatalDocument6 pagesIntl J Gynecology Obste - 2020 - Killeen - Examining The Use of The FIGO Nutrition Checklist in Routine AntenatalBenk Setsuna F. SeieiNo ratings yet
- RC Holy Spirit - Interact Club of Holy SpiritDocument3 pagesRC Holy Spirit - Interact Club of Holy Spiritrc_holyspiritNo ratings yet
- Chapter FiveDocument3 pagesChapter FiveSayp dNo ratings yet
- CMRT Position StatementDocument3 pagesCMRT Position StatementTito AlhoNo ratings yet
- Advocating For The Nursing RoleDocument6 pagesAdvocating For The Nursing Rolemp1757100% (1)
- Résumé Projet Mise en Place de Procédures de Sécurité en AnglaisDocument16 pagesRésumé Projet Mise en Place de Procédures de Sécurité en Anglaisgildas assandeNo ratings yet
- Ozempic Product Monograph PDFDocument59 pagesOzempic Product Monograph PDFAnonymous Complainer0% (1)
- Circulationaha 119 034512 PDFDocument19 pagesCirculationaha 119 034512 PDFNicola MaffeiNo ratings yet
- Health and Fitness Questions AnswersDocument3 pagesHealth and Fitness Questions AnswersĐình KhánhNo ratings yet
- MeningococcemiaDocument5 pagesMeningococcemiaErhiecka BasaNo ratings yet
- Bahasa Inggris Keperawatan DiarrheaDocument7 pagesBahasa Inggris Keperawatan DiarrheaNi Putu aristaNo ratings yet
- G o MS No 74Document13 pagesG o MS No 74snmpalanki7221100% (1)
- Exercise E F QDocument10 pagesExercise E F QCarol EleserioNo ratings yet
- Practical Gynecology 221002 234708Document44 pagesPractical Gynecology 221002 234708Muhammad RizgarNo ratings yet