You might also like
- Viability and Financial Assessment ReportDocument53 pagesViability and Financial Assessment ReportHazim Zakaria100% (2)
- Actuarial Methode Eng - 3Document51 pagesActuarial Methode Eng - 3Robot MarketingNo ratings yet
- Lecture 5Document38 pagesLecture 5ayladtlNo ratings yet
- Can We Afford Social Security and Medicare For 76 Million Boomers? (David C. John)Document14 pagesCan We Afford Social Security and Medicare For 76 Million Boomers? (David C. John)National Press FoundationNo ratings yet
- QN On Care of ElderlyDocument27 pagesQN On Care of ElderlyANITTA SNo ratings yet
- Lecture 9 - Social Insurance General ConceptsDocument19 pagesLecture 9 - Social Insurance General ConceptsCem DemirogluNo ratings yet
- Lec6 Dem Ins HandoutDocument41 pagesLec6 Dem Ins HandoutAnkita KumariNo ratings yet
- Questions SolutionsDocument11 pagesQuestions SolutionsKhurram Sadiq (Father Name:Muhammad Sadiq)No ratings yet
- Welfareeconomy2021 Chapter3Document46 pagesWelfareeconomy2021 Chapter3Kopija KopijaNo ratings yet
- PAY As You GoDocument11 pagesPAY As You GoCsapos DianaNo ratings yet
- Assignment: Course Code: STA101 Section: 05 Instructor: Mohammad Mastak Al Amin (MMA)Document10 pagesAssignment: Course Code: STA101 Section: 05 Instructor: Mohammad Mastak Al Amin (MMA)i CrYNo ratings yet
- Health Care: Sector ReportDocument16 pagesHealth Care: Sector Reportmona galalNo ratings yet
- Health Care Financing 2 (DR - Ali Gufron)Document25 pagesHealth Care Financing 2 (DR - Ali Gufron)Afra HanifiNo ratings yet
- Health InsuranceDocument54 pagesHealth InsuranceMinal DalviNo ratings yet
- Fiscal Measures by Goi: POST 1991Document69 pagesFiscal Measures by Goi: POST 1991Rajat VohraNo ratings yet
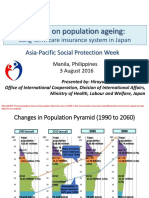
- APSP - Session 9A - Hiroyuki Yamaya - MHLWDocument8 pagesAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroNo ratings yet
- Tsa 95 V 477Document58 pagesTsa 95 V 477Ramón GutiérrezNo ratings yet
- 2181 French Dental Care InvestmentDocument5 pages2181 French Dental Care InvestmentolivierlevNo ratings yet
- Effects of 2022Document10 pagesEffects of 2022EstreLLA ValenciaNo ratings yet
- Politics of Social Health InsuranceDocument25 pagesPolitics of Social Health Insuranceperpustakaan pusatNo ratings yet
- Financing Options in Health Care 1Document13 pagesFinancing Options in Health Care 1Saurabh SumanNo ratings yet
- Financing Options in Health Care 1Document13 pagesFinancing Options in Health Care 1Saurabh SumanNo ratings yet
- COVID 19 Affecting Income Distribution in The EconomyDocument5 pagesCOVID 19 Affecting Income Distribution in The EconomyRonnie BerkovskyNo ratings yet
- Department of Labor and Employment HAZARD PAY GUIDELINESDocument6 pagesDepartment of Labor and Employment HAZARD PAY GUIDELINESChell Dela Peña CruzNo ratings yet
- Access To Health Care: 14. Serving CitizensDocument3 pagesAccess To Health Care: 14. Serving CitizensTalila SidaNo ratings yet
- Health Care Reform:: Update On Federal Efforts To Improve Access To Care For People Living With HIV/AIDSDocument28 pagesHealth Care Reform:: Update On Federal Efforts To Improve Access To Care For People Living With HIV/AIDSPeer Coach Academy ColoradoNo ratings yet
- Pension Provision in Germany - The First and Second Pillars in FocusDocument6 pagesPension Provision in Germany - The First and Second Pillars in FocuspensiontalkNo ratings yet
- Introduction PDFDocument55 pagesIntroduction PDFnilo biaNo ratings yet
- Unit 5 Social Security SchemesDocument58 pagesUnit 5 Social Security SchemesKanwaljeet SinghNo ratings yet
- ECON306 Mid Sem Test 2007 P HansenDocument5 pagesECON306 Mid Sem Test 2007 P HansenMobby Munyaradzi MuzamhindoNo ratings yet
- Sciencedirect: Is The Crop Insurance Program Effective in China? Evidence From Farmers Analysis in Five ProvincesDocument12 pagesSciencedirect: Is The Crop Insurance Program Effective in China? Evidence From Farmers Analysis in Five Provincesjeffrey aldayaNo ratings yet
- Long-Term Care in SpainDocument28 pagesLong-Term Care in SpainDavid HernandezNo ratings yet
- Cuaderno 6Document27 pagesCuaderno 6Inocente ReyesNo ratings yet
- Een Blauwdruk Voor Pensioenen. Genoeg Sparen, Goed Sparen en Slim Sparen (2017 Insurance Europe)Document44 pagesEen Blauwdruk Voor Pensioenen. Genoeg Sparen, Goed Sparen en Slim Sparen (2017 Insurance Europe)pensiontalkNo ratings yet
- BiondVax Corporate Presentation June 2018Document23 pagesBiondVax Corporate Presentation June 2018ChstdudeNo ratings yet
- Paying For Health CareDocument16 pagesPaying For Health CareUppala Sunil ChowdaryNo ratings yet
- Learning Journal Marco Unit 5Document3 pagesLearning Journal Marco Unit 5Lin YanNo ratings yet
- Health Status of Pakistan Jan 2014Document18 pagesHealth Status of Pakistan Jan 2014Dr.Abuzar ShiraniNo ratings yet
- France Healthcare SystemsDocument20 pagesFrance Healthcare SystemsRutvik GandhiNo ratings yet
- Health InsuranceDocument25 pagesHealth InsuranceTeresita Balgos100% (1)
- Social Health Protection Toward UHC in Lao PDRDocument16 pagesSocial Health Protection Toward UHC in Lao PDRADBI EventsNo ratings yet
- Employees' Health Insurance and Pension (Shakai Hoken 社会保険)Document2 pagesEmployees' Health Insurance and Pension (Shakai Hoken 社会保険)Putri HalinNo ratings yet
- The Lies They Tell About WelfareDocument2 pagesThe Lies They Tell About WelfareRichard AtkinsonNo ratings yet
- Health Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityDocument22 pagesHealth Care Models: International Comparisons: Dr. Jaime Llambías-Wolff, Ph.D. York UniversityTas SafetyTradeNo ratings yet
- Breaking The Poverty CycleDocument17 pagesBreaking The Poverty CyclePavan UNo ratings yet
- MONDAY EschtruthDocument51 pagesMONDAY EschtruthNational Press FoundationNo ratings yet
- Riplay Umum PaDocument8 pagesRiplay Umum ParfhazryyNo ratings yet
- Public Finance 10th Edition Rosen Test BankDocument7 pagesPublic Finance 10th Edition Rosen Test Bankrelatermotifef4oq100% (31)
- LTRAV2720 2017 Vanderborght SyllabusDocument45 pagesLTRAV2720 2017 Vanderborght Syllabuscorian.rikerNo ratings yet
- National Press Foundation Presentation On Reporting On Aging IssuesDocument28 pagesNational Press Foundation Presentation On Reporting On Aging IssuesNational Press FoundationNo ratings yet
- Tata AIA Life Insurance Non-Linked Comprehensive Health Rider (UIN: 110B031V02)Document28 pagesTata AIA Life Insurance Non-Linked Comprehensive Health Rider (UIN: 110B031V02)saravanaraj4uNo ratings yet
- Optimal Taxation in Overlapping Generations Economies With Aggregate RiskDocument95 pagesOptimal Taxation in Overlapping Generations Economies With Aggregate RiskpjNo ratings yet
- Final Exam Health EcnomimcDocument4 pagesFinal Exam Health EcnomimcLina AbuarqoubNo ratings yet
- Build Business Confidence Mobilizes Savings For Economics Development Security To Individuals Contribution To Social StabilityDocument17 pagesBuild Business Confidence Mobilizes Savings For Economics Development Security To Individuals Contribution To Social StabilityNisha NatarajanNo ratings yet
- Eco 631 Fall 2021 LW 4&5Document44 pagesEco 631 Fall 2021 LW 4&5johary2005No ratings yet
- Moving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of IndonesiaDocument32 pagesMoving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of IndonesiamochkurniawanNo ratings yet
- 3) Financial and Operational Performance Analysis 2018-2021Document33 pages3) Financial and Operational Performance Analysis 2018-2021Tomas LeonardelliNo ratings yet
- Social Insurance: Theoretical Foundations: Econ 231 - Public Finance Lectures 10 and 11Document20 pagesSocial Insurance: Theoretical Foundations: Econ 231 - Public Finance Lectures 10 and 11raphael_194352018No ratings yet
- Healthcare System in JapanDocument4 pagesHealthcare System in JapanBayuAkbarSyarifNo ratings yet
- Surviving the Aftermath of Covid-19:How Business Can Survive in the New EraFrom EverandSurviving the Aftermath of Covid-19:How Business Can Survive in the New EraNo ratings yet
- Consignment SalesDocument11 pagesConsignment SalesMaritess LobrigoNo ratings yet
- A Client S Conundrum 012507Document4 pagesA Client S Conundrum 012507Abhijit NaikNo ratings yet
- Telangana State Council of Higher Education: Provisional Allotment OrderDocument1 pageTelangana State Council of Higher Education: Provisional Allotment Orderrahul reddyNo ratings yet
- Bibliography & AnnexureDocument8 pagesBibliography & AnnexureNeeraj JainNo ratings yet
- What Is The Difference Between Bussiness Plan and Project ProposalDocument6 pagesWhat Is The Difference Between Bussiness Plan and Project ProposalshumetNo ratings yet
- Sales Consultant Agreement (164680) : Efu Life Assurance LTDDocument6 pagesSales Consultant Agreement (164680) : Efu Life Assurance LTDDheraj LalNo ratings yet
- Effects of Management Proficiency On Financial Performance of Foreign Commercial Bank, KenyaDocument7 pagesEffects of Management Proficiency On Financial Performance of Foreign Commercial Bank, Kenyavinay kumarNo ratings yet
- NRB Circulars 2066/67Document26 pagesNRB Circulars 2066/67Pasang LamaNo ratings yet
- Tugas Kelompok TM 3 Pengantar AkuntansiDocument4 pagesTugas Kelompok TM 3 Pengantar AkuntansiYuni ArtaNo ratings yet
- SkyLine Challan FormDocument1 pageSkyLine Challan Formaimsworld18No ratings yet
- PA 242.2 Problem Set 2Document2 pagesPA 242.2 Problem Set 2Laurence Niña X. OrtizNo ratings yet
- Civil Integrity AME StandardDocument3 pagesCivil Integrity AME Standarddhanu_lagwankarNo ratings yet
- VRL Project Report FinalDocument46 pagesVRL Project Report FinalSumitSalianNo ratings yet
- The Free Market (The Fifth Lesson)Document14 pagesThe Free Market (The Fifth Lesson)Himanshu Chawla100% (1)
- The Italian NPL Market Giugno 2020Document76 pagesThe Italian NPL Market Giugno 2020fadNo ratings yet
- Brand Loyalty and Customer Loyalty QuestionnaireDocument2 pagesBrand Loyalty and Customer Loyalty QuestionnaireAnonymous GhyLaqEcUUNo ratings yet
- Accounting 141 2020Document7 pagesAccounting 141 2020alexcharles433No ratings yet
- Functions of SIDBIDocument2 pagesFunctions of SIDBIRatnadeep MitraNo ratings yet
- Terms of Business For Cranleys Chartered Accountants As at 01 Janaury 2010Document14 pagesTerms of Business For Cranleys Chartered Accountants As at 01 Janaury 2010Colin DavisonNo ratings yet
- Syllabus CCB PDFDocument6 pagesSyllabus CCB PDFiamitgarg7No ratings yet
- Unit Viii - Audit of Equity Accounts T1 2014-2015 PDFDocument9 pagesUnit Viii - Audit of Equity Accounts T1 2014-2015 PDFSed ReyesNo ratings yet
- 1 Financial Markets - IntroductionDocument9 pages1 Financial Markets - IntroductionSergio Mirror MorenteNo ratings yet
- Iaa NotesDocument102 pagesIaa NotesSharan ReddyNo ratings yet
- Income Taxation TableDocument11 pagesIncome Taxation TableRomela Eleria GasesNo ratings yet
- 7 Finalnew Sugg June09Document17 pages7 Finalnew Sugg June09mknatoo1963No ratings yet
- Entrepreneurial Finance: Other Financing AlternativesDocument19 pagesEntrepreneurial Finance: Other Financing AlternativesAyan MohamedNo ratings yet
- HO & Branch AccountingDocument6 pagesHO & Branch AccountingMaria BeatriceNo ratings yet
- The Expert Guide To Affiliate MarketingDocument27 pagesThe Expert Guide To Affiliate MarketingViable SolutionsNo ratings yet
- Microbank: The Social Bank of "La Caixa"Document28 pagesMicrobank: The Social Bank of "La Caixa"joyNo ratings yet