You might also like
- Patient ReportDocument1 pagePatient ReportHimanshu MaheshwariNo ratings yet
- Complete - Report Check UpDocument1 pageComplete - Report Check UpBasil ShajiNo ratings yet
- P.NAGA LAKSHMI 57335-21 T3, T4+& +TSH+ (THYROID+PROFILE) 28 10 2021 20 50 22Document1 pageP.NAGA LAKSHMI 57335-21 T3, T4+& +TSH+ (THYROID+PROFILE) 28 10 2021 20 50 22VenuNo ratings yet
- Test ReportsDocument2 pagesTest ReportsChandrasekhara Reddy TNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSHDocument10 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSHkrishna prasadNo ratings yet
- Mrs Parveen Inamdar 29 02 2020 06 16 15 AM PDFDocument3 pagesMrs Parveen Inamdar 29 02 2020 06 16 15 AM PDFmalhari katakdoundNo ratings yet
- Report 2Document1 pageReport 2Muhammad HussainNo ratings yet
- Dneerajalaxmi 20220611120615333Document1 pageDneerajalaxmi 20220611120615333Donthula SripathiNo ratings yet
- B SRAVANI-Female16 Years-2090Document1 pageB SRAVANI-Female16 Years-2090vijaykumarNo ratings yet
- Laboratory Test Report: Mrs. Anusha TDocument1 pageLaboratory Test Report: Mrs. Anusha TAnu 1992No ratings yet
- Immunology: Iffat Ara Khandaker 50148371 16/10/2023 10:26AMDocument2 pagesImmunology: Iffat Ara Khandaker 50148371 16/10/2023 10:26AMMonotosh BiswasNo ratings yet
- Labreportnew - 2022-12-15T172158.070Document3 pagesLabreportnew - 2022-12-15T172158.070Himanshu MaheshwariNo ratings yet
- Dayo, Raymond Layugan 2284011329Document2 pagesDayo, Raymond Layugan 2284011329Raymond DayoNo ratings yet
- Labreportnew - 2022-12-17T172351.750Document1 pageLabreportnew - 2022-12-17T172351.750Himanshu MaheshwariNo ratings yet
- Vijaya Diagnostic Lab Report SummaryDocument10 pagesVijaya Diagnostic Lab Report SummaryJ SoujanyaNo ratings yet
- 012402260007_Ashok_PathDocument1 page012402260007_Ashok_Pathdyash1942No ratings yet
- Serum: MR M Edukondalu Kphb9502Document2 pagesSerum: MR M Edukondalu Kphb9502Edukondalu MorlaNo ratings yet
- Patient test results TSH and Free T4Document1 pagePatient test results TSH and Free T4Mohammad Dayyan KhanNo ratings yet
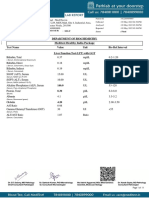
- Department of Chemical Pathology: Liver Function TestsDocument5 pagesDepartment of Chemical Pathology: Liver Function TestsmussadaqmakyNo ratings yet
- aga khan report resultDocument2 pagesaga khan report resultMuhammad Atif ShahNo ratings yet
- MR NITIN PDFDocument2 pagesMR NITIN PDFVenkat Nitin GuttaNo ratings yet
- Thyroid Profile: Laboratory Test ReportDocument1 pageThyroid Profile: Laboratory Test ReportArunsai Gilla100% (1)
- Vasavi Diagnostic Laboratory: Church Road, Chitradurga - 577501Document2 pagesVasavi Diagnostic Laboratory: Church Road, Chitradurga - 577501Vidya kiranNo ratings yet
- Department of LABORATORY MEDICINE: (Chemiluminescence)Document1 pageDepartment of LABORATORY MEDICINE: (Chemiluminescence)DivyaSNo ratings yet
- Dengue ReportDocument2 pagesDengue ReportLokesh RajNo ratings yet
- Woman's routine blood test reportDocument7 pagesWoman's routine blood test reportO TsukiNo ratings yet
- Chandan Diagnostic Centre: Department of BiochemistryDocument2 pagesChandan Diagnostic Centre: Department of BiochemistryRupal RupalNo ratings yet
- Lab Report: 2743025 LAB/20N/121831 27/jan/2022 Mr. Naman Thapliyal 13649512 StatusDocument2 pagesLab Report: 2743025 LAB/20N/121831 27/jan/2022 Mr. Naman Thapliyal 13649512 StatusM Abdul MoidNo ratings yet
- CH LAXMI-Female68 Years-1699Document2 pagesCH LAXMI-Female68 Years-1699vijaykumarNo ratings yet
- Uk007 2223 006609Document3 pagesUk007 2223 006609Arpit KumarNo ratings yet
- Laboratory Report Final: BiochemistryDocument1 pageLaboratory Report Final: BiochemistryAHAMED HUSSAINNo ratings yet
- Empeo, Veronica Anne Enriquez 2283027611Document2 pagesEmpeo, Veronica Anne Enriquez 2283027611Veronica Anne Enriquez EmpeoNo ratings yet
- Elevated Bilirubin Test ResultsDocument1 pageElevated Bilirubin Test ResultsGeraldyn IdoNo ratings yet
- GC129053 (1) - 210804 - 061549Document2 pagesGC129053 (1) - 210804 - 061549anuragNo ratings yet
- 19 Dec 2022Document1 page19 Dec 2022Yogesh ArasuNo ratings yet
- LabreportnewDocument2 pagesLabreportnewbs8403226No ratings yet
- Thyroid function test report for 18-year old maleDocument2 pagesThyroid function test report for 18-year old malearjun guptaNo ratings yet
- ReportDocument1 pageReportMohd IshaqNo ratings yet
- Result Entry ReportDocument1 pageResult Entry ReportMaggidi vaishnaviNo ratings yet
- Laboratory Report Final: BiochemistryDocument4 pagesLaboratory Report Final: BiochemistrygayathridevikgNo ratings yet
- KG195124 PDFDocument3 pagesKG195124 PDFJyothi NairNo ratings yet
- Manaloto, Cid Marlon Libo 2211108539Document3 pagesManaloto, Cid Marlon Libo 2211108539Camille Marie ManalotoNo ratings yet
- ItsOurBaby File-2Document5 pagesItsOurBaby File-2AA4884No ratings yet
- PawanVerma 189810Document11 pagesPawanVerma 189810Shivam verma OfficialNo ratings yet
- Hormone Assay Result Bio. Ref. Interval Unit TestDocument1 pageHormone Assay Result Bio. Ref. Interval Unit TestToushik Ahamed MollaNo ratings yet
- Haematology Test Result Unit Biological Ref. Interval Prothrombin TimeDocument6 pagesHaematology Test Result Unit Biological Ref. Interval Prothrombin TimeNidhi RakeshNo ratings yet
- Liver Function Test ResultsDocument1 pageLiver Function Test Resultssolid_impactNo ratings yet
- Naveen Ramesh 21012022Document1 pageNaveen Ramesh 21012022Naveen BalajiNo ratings yet
- Yzdg1707Document2 pagesYzdg1707Ashvik AnumakondaNo ratings yet
- Department of Laboratory Medicine: (Chemiluminescence)Document1 pageDepartment of Laboratory Medicine: (Chemiluminescence)DivyaSNo ratings yet
- Jothi Ganesan-Female55-2593Document1 pageJothi Ganesan-Female55-2593karunamoorthyNo ratings yet
- FinalDocument3 pagesFinalAnupam Saraf IINo ratings yet
- Investigation Biological Reference Interval Observed Value UnitDocument2 pagesInvestigation Biological Reference Interval Observed Value Unitsrividya nagarajanNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Total T3Document3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Total T3Chandu Chan LyristNo ratings yet
- Mrs. Rani's thyroid stimulating hormone test resultsDocument1 pageMrs. Rani's thyroid stimulating hormone test resultsHimanshu MaheshwariNo ratings yet
- Final: Patient Name: Neetu 0009XC011564 Ref. DoctorDocument1 pageFinal: Patient Name: Neetu 0009XC011564 Ref. Doctorpiyush882676No ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- Mr. Ravi ChopraDocument1 pageMr. Ravi ChopraRavi ChopraNo ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- Marriage BiodataDocument1 pageMarriage BiodataSid VohraNo ratings yet
- How To Draw Line With Angle and Distance in AutocadDocument1 pageHow To Draw Line With Angle and Distance in AutocadSid VohraNo ratings yet
- HIV Test Results for Mr. Ravi BishtDocument1 pageHIV Test Results for Mr. Ravi BishtSid VohraNo ratings yet
- Krishna Sharma Salary Slip-NOVDocument1 pageKrishna Sharma Salary Slip-NOVSid VohraNo ratings yet
- Pay Slip For October 2019: Amplifon India Private LimitedDocument1 pagePay Slip For October 2019: Amplifon India Private LimitedSid VohraNo ratings yet
- Keventers (A Unit of Super Milk Products PVT - LTD) : Payslip For The Month of February 2019Document1 pageKeventers (A Unit of Super Milk Products PVT - LTD) : Payslip For The Month of February 2019Sid VohraNo ratings yet
- Patton, C. Sanchez-Eppler, B. (Editors) (2000) - Queer DiasporasDocument317 pagesPatton, C. Sanchez-Eppler, B. (Editors) (2000) - Queer Diasporastutkjhf0% (1)
- Pre AnestesiDocument64 pagesPre AnestesiKevin YonathanNo ratings yet
- Actualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley MonkDocument35 pagesActualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley Monkinfo7615No ratings yet
- Glasgow Coma Scale Canvas NCM 116 SkillsDocument6 pagesGlasgow Coma Scale Canvas NCM 116 Skillsbing bongNo ratings yet
- Patient: Transthoracic Echocardiography ReportDocument2 pagesPatient: Transthoracic Echocardiography Reportluh sriaryantiNo ratings yet
- Lazarus Basid IDDocument7 pagesLazarus Basid IDmiji_ggNo ratings yet
- Consanguinity Tulyagotriya Vivaha Impact On Child Health A Review LiteratureDocument4 pagesConsanguinity Tulyagotriya Vivaha Impact On Child Health A Review LiteratureEditor IJTSRDNo ratings yet
- Promote Near-Miss ReportingDocument57 pagesPromote Near-Miss Reportingmalik jahan93% (14)
- Understanding The Self: Sexual SelfDocument13 pagesUnderstanding The Self: Sexual SelfJustin UyNo ratings yet
- Challenges Implementing Telemedicine in AfghanistanDocument6 pagesChallenges Implementing Telemedicine in AfghanistanMuhibullah AmanNo ratings yet
- Male Genitalia AbnormalitiesDocument25 pagesMale Genitalia AbnormalitiesClaudette Kyle CornelioNo ratings yet
- Tugas Aplikasi K3 Di Rumah SakitDocument6 pagesTugas Aplikasi K3 Di Rumah SakitSyifa marha GhaisaniNo ratings yet
- Original Article: Genetic Inheritance Pattern in Prurigo HebraDocument6 pagesOriginal Article: Genetic Inheritance Pattern in Prurigo HebraTaufiq AkbarNo ratings yet
- Bcga 2003 Code of Practice CP 34Document58 pagesBcga 2003 Code of Practice CP 34wssengltdNo ratings yet
- Fruit EssayDocument10 pagesFruit EssayHerald Jay Herrera BautistaNo ratings yet
- The Impact of DHIS 2 in Kenya - A User PerspectiveDocument12 pagesThe Impact of DHIS 2 in Kenya - A User PerspectiveJames GathogoNo ratings yet
- How To Ensure Safety For Castable MixingDocument4 pagesHow To Ensure Safety For Castable MixingNaelNo ratings yet
- Jurnal MFSDocument11 pagesJurnal MFSAfni YusnitaNo ratings yet
- Sterilization of Operation Theatres - Time To Stop FumigationDocument2 pagesSterilization of Operation Theatres - Time To Stop Fumigationtummalapalli venkateswara rao100% (1)
- Breathing Pattern Assessment and InterventionDocument3 pagesBreathing Pattern Assessment and InterventionAziil LiizaNo ratings yet
- ACFrOgA8Wr6yi7FYY4jC6qYdMj86L225Chgo2d G IA93LyTlqzSvhwFKSNqF61OaWxP3w9EULJvRjQb3oNc5 YaEr 21n-4c0MdfvCp85bfDDtw5zQefV2SHbOfDZQDocument8 pagesACFrOgA8Wr6yi7FYY4jC6qYdMj86L225Chgo2d G IA93LyTlqzSvhwFKSNqF61OaWxP3w9EULJvRjQb3oNc5 YaEr 21n-4c0MdfvCp85bfDDtw5zQefV2SHbOfDZQShaina MabborangNo ratings yet
- Drug Study: Pharmacologic AlDocument7 pagesDrug Study: Pharmacologic AlFrudz Orjaleza100% (1)
- 440 - Full Manuscript-928-1-10-20220825Document8 pages440 - Full Manuscript-928-1-10-20220825Đăng QuânNo ratings yet
- Hydrochloric Acid 30-35%Document17 pagesHydrochloric Acid 30-35%Wong Peng ChiongNo ratings yet
- Irc Squat ClinicDocument52 pagesIrc Squat Clinicapi-238394171No ratings yet
- JCM 11 00011Document11 pagesJCM 11 00011Lal NandaniNo ratings yet
- Minutes 1ST Spta Gen. MeetingDocument3 pagesMinutes 1ST Spta Gen. MeetingMarco Alfonzo100% (1)
- Government SchemesDocument86 pagesGovernment Schemesanon_462060725No ratings yet
- Introduction To Patient SafetyDocument54 pagesIntroduction To Patient Safetyrejoicedear2020No ratings yet
- Plagiarism - Paraphrase and Summary HandoutDocument10 pagesPlagiarism - Paraphrase and Summary HandoutTika VirginiyaNo ratings yet