You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Zhang - Synopsis of The Golden Cabinet With 300 CasesDocument566 pagesZhang - Synopsis of The Golden Cabinet With 300 CasesMarshall100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
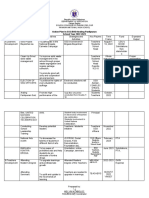
- Action Plan in SSG/BKD/Araling Panlipunan School Year 2022-2023Document3 pagesAction Plan in SSG/BKD/Araling Panlipunan School Year 2022-2023Melvin Aboloc100% (2)
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesMelvin AbolocNo ratings yet
- Department of Education: Republic of The P HilippinesDocument6 pagesDepartment of Education: Republic of The P HilippinesMelvin AbolocNo ratings yet
- Grade 10 Silver Class Program: Department of EducationDocument5 pagesGrade 10 Silver Class Program: Department of EducationMelvin AbolocNo ratings yet
- Excel Structuring 2019Document257 pagesExcel Structuring 2019Melvin AbolocNo ratings yet
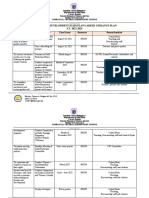
- Gender and Development (Gad) Plan/Career Guidance Plan S.Y. 2022-2023Document3 pagesGender and Development (Gad) Plan/Career Guidance Plan S.Y. 2022-2023Melvin Aboloc100% (1)
- Individual Learning Monitoring PlanDocument26 pagesIndividual Learning Monitoring PlanMelvin AbolocNo ratings yet
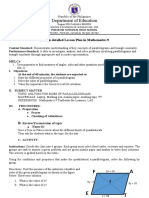
- Department of Education: A Semi-Detailed Lesson Plan in Mathematics 9Document3 pagesDepartment of Education: A Semi-Detailed Lesson Plan in Mathematics 9Melvin AbolocNo ratings yet
- Listening Jahshan OET CollectionDocument194 pagesListening Jahshan OET CollectionAKHILNo ratings yet
- A Systematic Review of The Systematic Review of Post COVID-19 SyndromeDocument6 pagesA Systematic Review of The Systematic Review of Post COVID-19 Syndromeeditorial.boardNo ratings yet
- Food Safety Module - WorkbookDocument51 pagesFood Safety Module - WorkbookHerman SmitNo ratings yet
- Proposal 1 CorrectionDocument53 pagesProposal 1 Correctionkrfnxgg krfnxggNo ratings yet
- Examination of Thyroid Swelling and CASE DR Manas MRS SurgeryDocument10 pagesExamination of Thyroid Swelling and CASE DR Manas MRS SurgeryManas RanjanNo ratings yet
- Erik Van Woensel Classical Homeopathy Evidence Based Medicine Vol. 2Document23 pagesErik Van Woensel Classical Homeopathy Evidence Based Medicine Vol. 2Sohail LatifNo ratings yet
- Psychosomatic Pain: Ertuğrul AllahverdiDocument20 pagesPsychosomatic Pain: Ertuğrul AllahverdidiasNo ratings yet
- Transforming SubjectivitiesDocument35 pagesTransforming SubjectivitiesIndra GunawanNo ratings yet
- Lot 6 Block 6 Sta. Catalina Homes Tabing IlogDocument12 pagesLot 6 Block 6 Sta. Catalina Homes Tabing IlogAina De LeonNo ratings yet
- PPPD Is On A Spectrum in The General PopulationDocument11 pagesPPPD Is On A Spectrum in The General PopulationJuan Hernández GarcíaNo ratings yet
- A) Normal Referral Letter:: Most Likely, Grave's DiseaseDocument8 pagesA) Normal Referral Letter:: Most Likely, Grave's DiseaseSyed Danish AliNo ratings yet
- Declaration With Regard To Medical Fitness:: Vamsi Talachintala T.Vamsi Witness: (Name & Address)Document2 pagesDeclaration With Regard To Medical Fitness:: Vamsi Talachintala T.Vamsi Witness: (Name & Address)Prem sagarNo ratings yet
- Summary of Findings Conclusions and RecommendationsDocument13 pagesSummary of Findings Conclusions and RecommendationsCharisma PastorNo ratings yet
- Kalibo Rural Health Unit Vi AklanDocument3 pagesKalibo Rural Health Unit Vi AklanSam Blaccpink IINo ratings yet
- Theoretical Reflections of Leininger's Cross-Cultural Care in The Context of Covid-19Document10 pagesTheoretical Reflections of Leininger's Cross-Cultural Care in The Context of Covid-19ailyn pinedaNo ratings yet
- Somatic Symptom Disorder: Placer, Selorio & VuelgaDocument52 pagesSomatic Symptom Disorder: Placer, Selorio & Vuelgacarsheen claireNo ratings yet
- To Screening For Referral in Physical Therapy: DR Sumaira YasminDocument24 pagesTo Screening For Referral in Physical Therapy: DR Sumaira YasminM TVNo ratings yet
- C.F. Sharp Crew Management Inc vs. Legal Heirs of The Late Godofredo RepisoDocument35 pagesC.F. Sharp Crew Management Inc vs. Legal Heirs of The Late Godofredo Repisorodel talabaNo ratings yet
- Contingency Plan of Mambagaton Farm School 1Document28 pagesContingency Plan of Mambagaton Farm School 1Jewelden MayanNo ratings yet
- Name:-Lavkumar Narendrabhai Patel ENROLLMENT NO.: - 190160116087 Subject: - Ai Practicals Branch: - It (A3) EmailDocument51 pagesName:-Lavkumar Narendrabhai Patel ENROLLMENT NO.: - 190160116087 Subject: - Ai Practicals Branch: - It (A3) EmailasdNo ratings yet
- New Covid Variant Xe Symptoms - Google SearchDocument1 pageNew Covid Variant Xe Symptoms - Google SearchjetaNo ratings yet
- Chen 2006Document6 pagesChen 2006Rahmat MitorolaNo ratings yet
- Supw Project Work 2021-2022: Done By: Haswanth Class: 12 DDocument64 pagesSupw Project Work 2021-2022: Done By: Haswanth Class: 12 DMekala HaswanthNo ratings yet
- Migraine - Symptoms, Causes, Treatment, Triggers, and MoreDocument35 pagesMigraine - Symptoms, Causes, Treatment, Triggers, and MoreKarlla SuarezNo ratings yet
- Part C - Multiple SclerosisDocument4 pagesPart C - Multiple SclerosisStaph AureusNo ratings yet
- LBM-Secrets of Black MarshDocument35 pagesLBM-Secrets of Black MarshSamuel SacherNo ratings yet
- Cervico-Cranial Red Flag Tool - Final For SoMeDocument1 pageCervico-Cranial Red Flag Tool - Final For SoMeDavid StreisselNo ratings yet
- Sensations in HomoeopathyDocument1,043 pagesSensations in HomoeopathyEkta Tiwary100% (3)
- Comparative Study of The Academic Stress and Anxiety Among Working and Non-Working College StudentsDocument157 pagesComparative Study of The Academic Stress and Anxiety Among Working and Non-Working College StudentsGallego MianNo ratings yet