You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Referee Report TemplateDocument3 pagesReferee Report TemplateTiyas Prasetya Kusumaningrum100% (2)
- Determination of The Capitalization Values For No Load Losses and Load LossesDocument12 pagesDetermination of The Capitalization Values For No Load Losses and Load LossesSaman GamageNo ratings yet
- Self-Assessment ReportDocument63 pagesSelf-Assessment ReportTiyas Prasetya KusumaningrumNo ratings yet
- ASIIN International Conference 2018 ProgrammeDocument7 pagesASIIN International Conference 2018 ProgrammeTiyas Prasetya KusumaningrumNo ratings yet
- Criteria For The Accreditation of Degree Programmes ASIIN Quality SealDocument33 pagesCriteria For The Accreditation of Degree Programmes ASIIN Quality SealTiyas Prasetya KusumaningrumNo ratings yet
- Letters To The EditorDocument5 pagesLetters To The EditorTiyas Prasetya KusumaningrumNo ratings yet
- Case Study of Master of Business AdminisDocument8 pagesCase Study of Master of Business AdminisYoke MalondaNo ratings yet
- Navigating The Complexities of Modern SocietyDocument2 pagesNavigating The Complexities of Modern SocietytimikoNo ratings yet
- Pearson Type IV Characteristic Function 1196285389Document9 pagesPearson Type IV Characteristic Function 1196285389peppas4643No ratings yet
- Nibrt Training 2023 FinalDocument50 pagesNibrt Training 2023 FinalAbdelrahman Ali OsmanNo ratings yet
- Uw Math Stat394 Hw4 SolDocument4 pagesUw Math Stat394 Hw4 SolRizsNo ratings yet
- DESIGN AND ANALYSIS OF HYDRAULIC POWERPACK AND PUMcalculationsDocument10 pagesDESIGN AND ANALYSIS OF HYDRAULIC POWERPACK AND PUMcalculationssubhasNo ratings yet
- BS en 14024-2004 Thermal BreakDocument32 pagesBS en 14024-2004 Thermal BreakGlenn LamboNo ratings yet
- Presentation Progress and Status of Consulting Services ContractDocument26 pagesPresentation Progress and Status of Consulting Services ContractDjoko SubektiNo ratings yet
- Polartek Plus Eeac331Document84 pagesPolartek Plus Eeac331Sodel MezaNo ratings yet
- Statisticsprobability11 q4 Week2 v4Document10 pagesStatisticsprobability11 q4 Week2 v4Sheryn CredoNo ratings yet
- REELY Chapter 7 Flashcards - QuizletDocument2 pagesREELY Chapter 7 Flashcards - QuizletCERTIFIED TROLLNo ratings yet
- Application of Spatial Technology in Mal PDFDocument8 pagesApplication of Spatial Technology in Mal PDFdevNo ratings yet
- Biological PlausibilityDocument2 pagesBiological PlausibilityTreeSix SolutionsNo ratings yet
- 2019jahh 22 447GDocument12 pages2019jahh 22 447GTomi DwiNo ratings yet
- Training Evaluation Form: Seven Seas HotelDocument2 pagesTraining Evaluation Form: Seven Seas HotelPiyush SevenseasNo ratings yet
- DRU#1 Engineering Meeting Minutes 12-04-14 - 004Document3 pagesDRU#1 Engineering Meeting Minutes 12-04-14 - 004vsnaiduqcNo ratings yet
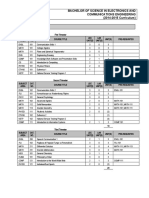
- Program Structure: Bachelor of Science in Electronics and Communications Engineering (2014-2015 Curriculum)Document5 pagesProgram Structure: Bachelor of Science in Electronics and Communications Engineering (2014-2015 Curriculum)Zainab KadhemNo ratings yet
- 1.3. Intention of This StudyDocument1 page1.3. Intention of This StudyJack FrostNo ratings yet
- Lesson 1 MATHEMATICS IN THE MODERN WORLDDocument39 pagesLesson 1 MATHEMATICS IN THE MODERN WORLDericacatu3No ratings yet
- FormulaShell SAE 10W 40 Motor Oil DatasheetDocument3 pagesFormulaShell SAE 10W 40 Motor Oil DatasheetAnonymous YjoCCKNo ratings yet
- 10) Assessment On Performance and Challenges of EthiopianDocument11 pages10) Assessment On Performance and Challenges of EthiopianyaregalNo ratings yet
- Construction Site & Lifting by CraneDocument68 pagesConstruction Site & Lifting by CraneShammas RajputNo ratings yet
- Motivation TheoriesDocument26 pagesMotivation TheoriesShalin Subba LimbuNo ratings yet
- Popular Horoscopes and The "Barnum Effect" PDFDocument12 pagesPopular Horoscopes and The "Barnum Effect" PDFYilbert Oswaldo Jimenez CanoNo ratings yet
- Chapter 3 Issues On Human DevelopmentDocument25 pagesChapter 3 Issues On Human DevelopmentJheny Palamara75% (4)
- Designing User-Centered Decision Support Tools For AgricultureDocument17 pagesDesigning User-Centered Decision Support Tools For AgricultureCABINo ratings yet
- Factoring Perfect Square Trinomials: Lesson 4Document29 pagesFactoring Perfect Square Trinomials: Lesson 4Jessa A.No ratings yet
- CBSE Class 10 Light Reflection and Refraction Study NotesDocument19 pagesCBSE Class 10 Light Reflection and Refraction Study NotesKanchana SriramuluNo ratings yet
- Role of Geotechnical Properties of Soil On Civil Engineering StructuresDocument8 pagesRole of Geotechnical Properties of Soil On Civil Engineering StructuresSaša MarinNo ratings yet