You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Service Blueprint HospitalDocument1 pageService Blueprint HospitalRaghav R Chawla40% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
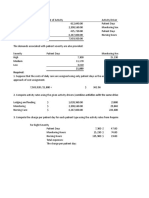
- ABC, Resource Drivers, Service Industry Glencoe Medical Clinic Operates A Cardiology Care Unit and A Maternity Care UnitDocument3 pagesABC, Resource Drivers, Service Industry Glencoe Medical Clinic Operates A Cardiology Care Unit and A Maternity Care UnitKailash KumarNo ratings yet
- Historical Evolution of Nursing ResearchDocument9 pagesHistorical Evolution of Nursing ResearchGayathri R100% (2)
- Assessment Scientific Analysis Planning Intervention Rationale Evaluation Short Term GoalDocument4 pagesAssessment Scientific Analysis Planning Intervention Rationale Evaluation Short Term GoalJayson OlileNo ratings yet
- 1,000 Questions To Help You Pass The Emergency Medicine BoardsDocument338 pages1,000 Questions To Help You Pass The Emergency Medicine Boardseric91% (11)
- Fetal Cerebro-Placental Ratio and Adverse Perinatal Outcome: Systematic Review and Meta-Analysis of The Association and Diagnostic PerformanceDocument8 pagesFetal Cerebro-Placental Ratio and Adverse Perinatal Outcome: Systematic Review and Meta-Analysis of The Association and Diagnostic Performancebidan22No ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument15 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive Biologybidan22No ratings yet
- Diagnostics 07 00012Document10 pagesDiagnostics 07 00012bidan22No ratings yet
- AmniotomiDocument8 pagesAmniotomibidan22No ratings yet
- Menopause Hormone Replacement TherapyDocument4 pagesMenopause Hormone Replacement Therapybidan22No ratings yet
- Abnormal Vaginal Bleeding Policar 051611Document69 pagesAbnormal Vaginal Bleeding Policar 051611bidan22No ratings yet
- Early Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical TrialDocument5 pagesEarly Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical Trialbidan22No ratings yet
- Antiphospholipid Antibody Syndrome and PregnancyDocument17 pagesAntiphospholipid Antibody Syndrome and Pregnancybidan22No ratings yet
- Contingency Plan For Covid - 19Document12 pagesContingency Plan For Covid - 19anneNo ratings yet
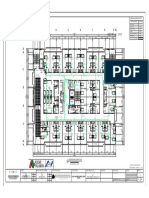
- ACE PALAWAN MGAS-SIXTH FLOOR-ModelDocument1 pageACE PALAWAN MGAS-SIXTH FLOOR-ModelBerlin Andrew SionNo ratings yet
- Diploma Entrants Admissions List 2018 2019 PDFDocument15 pagesDiploma Entrants Admissions List 2018 2019 PDFAyesigwa Gerald96No ratings yet
- Resume Kelsi WeakleyDocument2 pagesResume Kelsi Weakleyapi-276879599No ratings yet
- Maintaining Fluid Balance: Barbara WorkmanDocument8 pagesMaintaining Fluid Balance: Barbara WorkmanNurul HendrianiNo ratings yet
- MKT-PK3-01-01 Identifikasi, Penilaian & Pengendalian RisikoDocument3 pagesMKT-PK3-01-01 Identifikasi, Penilaian & Pengendalian RisikoDania RachmawatiNo ratings yet
- Nejmoa1611593 AppendixDocument43 pagesNejmoa1611593 AppendixFasihaNo ratings yet
- Radiographs in Prosthodontics / Orthodontic Courses by Indian Dental AcademyDocument38 pagesRadiographs in Prosthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (4)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsAshok KumarNo ratings yet
- Nurse To Nurse Bedside Shift Report LB 5th WeekDocument12 pagesNurse To Nurse Bedside Shift Report LB 5th Weekapi-527286440No ratings yet
- RSMPD Abstract E-BookDocument185 pagesRSMPD Abstract E-BookjesslinaNo ratings yet
- Questions For NursingDocument26 pagesQuestions For Nursingjoan olanteNo ratings yet
- Adverse Drug Reaction Monitoring Reporting PDFDocument3 pagesAdverse Drug Reaction Monitoring Reporting PDFRossana Rizqita PutriNo ratings yet
- Condylomata AcuminataDocument10 pagesCondylomata Acuminataalejandro fernandezNo ratings yet
- Guidelines Made Simple Chest PainDocument18 pagesGuidelines Made Simple Chest PainPaul JohnNo ratings yet
- Post ExamDocument7 pagesPost ExamJean Cuenta0% (1)
- The Safe Use of Syringe Driver in Palliative CareDocument3 pagesThe Safe Use of Syringe Driver in Palliative CarecohenserbanNo ratings yet
- Practical Application of Statistics in NursingDocument3 pagesPractical Application of Statistics in NursingApong JuanNo ratings yet
- Theories of AgingDocument2 pagesTheories of AgingJeremiah JustoNo ratings yet
- Listening - Sample 1Document15 pagesListening - Sample 1Mamdouh GallowNo ratings yet
- Restorative Dentistry: " The Sandwich Technique "Document11 pagesRestorative Dentistry: " The Sandwich Technique "Asya Mubarak100% (1)
- Public Health Informatics and GISDocument52 pagesPublic Health Informatics and GISNise Mon KuriakoseNo ratings yet
- Detailed Lesson Plan in Health 9Document6 pagesDetailed Lesson Plan in Health 9marvierose0% (1)
- Concept Communicable DiseasesDocument477 pagesConcept Communicable DiseasesrimeoznekNo ratings yet
- An Overview of Asthma Management - UpToDateDocument83 pagesAn Overview of Asthma Management - UpToDatedocjime9004No ratings yet