You might also like
- ACC SAP 8 Exam1&2ACC SAP 8 Exam1&2Document115 pagesACC SAP 8 Exam1&2ACC SAP 8 Exam1&2Yahya Hassan Hussein El-tamaly100% (3)
- The Zwolftonspiel of Josef Matthias Hauer: John RDocument36 pagesThe Zwolftonspiel of Josef Matthias Hauer: John RMax Kühn100% (1)
- SUCCESSION CHAMP Notes (BALANE)Document91 pagesSUCCESSION CHAMP Notes (BALANE)carlee01483% (6)
- Nursing Care PlanDocument12 pagesNursing Care Planzsazsageorge86% (21)
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030No ratings yet
- Developing Managers and LeadersDocument48 pagesDeveloping Managers and LeadersMazen AlbsharaNo ratings yet
- Conversation LaundryDocument2 pagesConversation Laundryvanni octavania88% (8)
- The People of The Materia Medica World: A Comparative Materia Medica Part-1Document5 pagesThe People of The Materia Medica World: A Comparative Materia Medica Part-1Paromita Dasgupta50% (2)
- Hormone Therapy and Cardiovascular DiseaseDocument7 pagesHormone Therapy and Cardiovascular Diseaseosama saeedNo ratings yet
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiNo ratings yet
- StrokeDocument67 pagesStrokeGagi MiloševićNo ratings yet
- Association Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitDocument5 pagesAssociation Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitIOSRjournalNo ratings yet
- Review Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersDocument22 pagesReview Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersNnaemeka NwobodoNo ratings yet
- An Update On Menopausal Hormone Replacement Therapy in Women and Cardiovascular DiseaseDocument8 pagesAn Update On Menopausal Hormone Replacement Therapy in Women and Cardiovascular DiseaseAlmas TNo ratings yet
- Effects DMCEA01Document11 pagesEffects DMCEA01milmrch523No ratings yet
- Pre Eclampsia and Risk of Cardiovascular Disease and CancerDocument12 pagesPre Eclampsia and Risk of Cardiovascular Disease and CancerDjanino FernandesNo ratings yet
- Association of Variability in Uric Acid and Future CliDocument7 pagesAssociation of Variability in Uric Acid and Future Clinguyenthanhluan2801No ratings yet
- Rosuvastatia y PCR en ScaDocument3 pagesRosuvastatia y PCR en ScaWilliankmachoNo ratings yet
- UKPDS36Document8 pagesUKPDS36Siskawati SuparminNo ratings yet
- Serum Uric Acid Level in Acute Stroke Patients: Original ResearchDocument7 pagesSerum Uric Acid Level in Acute Stroke Patients: Original ResearchJoseph Sipiran ReyesNo ratings yet
- Jurnal 1Document10 pagesJurnal 1fitri juliantiNo ratings yet
- Role of Hypertension and Obesity As Risk Factors For IhdDocument5 pagesRole of Hypertension and Obesity As Risk Factors For IhdMohammad Mujtaba GhaffariNo ratings yet
- Gender Differences in Ischemic Heart Disease: Ryotaro Wake and Minoru YoshiyamaDocument7 pagesGender Differences in Ischemic Heart Disease: Ryotaro Wake and Minoru YoshiyamaChirag ParmarNo ratings yet
- Module 1 - Sample PaperDocument7 pagesModule 1 - Sample PaperknuckleheadNo ratings yet
- 1 Running Head: Preventing Recurrent Myocardial InfarctionsDocument10 pages1 Running Head: Preventing Recurrent Myocardial InfarctionsIsaacNo ratings yet
- Sankar D NaveenthanDocument10 pagesSankar D NaveenthanDr. Jatin GargNo ratings yet
- R245 FullDocument11 pagesR245 FullYuliana WiralestariNo ratings yet
- 2019 Article 612Document17 pages2019 Article 612Asad NawazNo ratings yet
- Association Between Heart Disease in Pregnancy With Cardiac EventsDocument7 pagesAssociation Between Heart Disease in Pregnancy With Cardiac EventsAsri Mukti NantaNo ratings yet
- Ference BA Et Al. N Eng J Med 2016Document56 pagesFerence BA Et Al. N Eng J Med 2016Juan Manuel UrbanoNo ratings yet
- Nejm Pcsk9 StudyDocument10 pagesNejm Pcsk9 Studyherbertgur777No ratings yet
- 974 Full PDFDocument12 pages974 Full PDFsugamilasNo ratings yet
- Cystatin C GambarDocument12 pagesCystatin C GambarMaya RustamNo ratings yet
- Serum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenDocument15 pagesSerum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenEcha MagungNo ratings yet
- Ioakeimidis2016Document9 pagesIoakeimidis2016EnzoNo ratings yet
- Women and Diabetes Preventing Heart Disease in A New Era of TherapiesDocument13 pagesWomen and Diabetes Preventing Heart Disease in A New Era of TherapiesWilliam Ricardo Effio GalvezNo ratings yet
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDocument17 pagesCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNo ratings yet
- The M235T Single Nucleotide Polymorphism in The Angiotensinogen Gene Is Associated With Calcium in Patients With A Family History ofDocument4 pagesThe M235T Single Nucleotide Polymorphism in The Angiotensinogen Gene Is Associated With Calcium in Patients With A Family History ofpicolina_92No ratings yet
- Research Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionDocument9 pagesResearch Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionmikeNo ratings yet
- Risk Related To Hormone Therapy and Cardiovascular Disease in WomenDocument44 pagesRisk Related To Hormone Therapy and Cardiovascular Disease in Womenosama saeedNo ratings yet
- Cme - NisaDocument12 pagesCme - Nisanadya shabirah zahraNo ratings yet
- Hubungan Rasio Trigliserida/High Density Lipoprotein-Cholesterol (TG/HDL-C) Dengan Kejadian Infark Miokard Akut Di RSUP Prof. Dr. R. D. Kandou ManadoDocument5 pagesHubungan Rasio Trigliserida/High Density Lipoprotein-Cholesterol (TG/HDL-C) Dengan Kejadian Infark Miokard Akut Di RSUP Prof. Dr. R. D. Kandou ManadoIvanna NdoenNo ratings yet
- Advances in Anesthesia: Optimal Perioperative Blood Pressure ManagementDocument13 pagesAdvances in Anesthesia: Optimal Perioperative Blood Pressure Managementfabian arassiNo ratings yet
- CEAAAADocument12 pagesCEAAAAfikebatuNo ratings yet
- Jurnal Internasional Peb Nifas 5Document10 pagesJurnal Internasional Peb Nifas 5Herdian KurniawanNo ratings yet
- Appelman - Sex Differences in Cardiovascular Risk Factors - 2015Document8 pagesAppelman - Sex Differences in Cardiovascular Risk Factors - 2015MIRIAM VIDURRIZAGANo ratings yet
- Hormone Replacement HerapyDocument5 pagesHormone Replacement HerapyCindy HartNo ratings yet
- Journal Medicine: The New EnglandDocument9 pagesJournal Medicine: The New EnglandFernanda Araújo AvendanhaNo ratings yet
- JCH 12758Document6 pagesJCH 12758HanafieHeluthNo ratings yet
- 2017-Taravatmanesh, Et Al-2017 - Determining The Factors Associated With Cardiovascular Disease Recurrence Tehran Lipid and Glucose StudyDocument7 pages2017-Taravatmanesh, Et Al-2017 - Determining The Factors Associated With Cardiovascular Disease Recurrence Tehran Lipid and Glucose Studycipto susiloNo ratings yet
- Age-Related Longitudinal Change in Cardiac Structure and Function in Adults at Increased Cardiovascular RiskDocument18 pagesAge-Related Longitudinal Change in Cardiac Structure and Function in Adults at Increased Cardiovascular Riskabraham rumayaraNo ratings yet
- Human C-Reactive Protein and The Metabolic SyndromeDocument13 pagesHuman C-Reactive Protein and The Metabolic SyndromeEmir SaricNo ratings yet
- The Impact of Serum Uric Acid On Cardiovascular OutcomesDocument9 pagesThe Impact of Serum Uric Acid On Cardiovascular OutcomestinatobingNo ratings yet
- 116 229 1 SMDocument6 pages116 229 1 SMsinlookerNo ratings yet
- Stroke PDFDocument67 pagesStroke PDFBadrul MunirNo ratings yet
- ALGER 28 04 2023 Version Courte Version 03Document93 pagesALGER 28 04 2023 Version Courte Version 03zakaribitcoinNo ratings yet
- Literature Review On Acute Coronary SyndromeDocument7 pagesLiterature Review On Acute Coronary Syndromegazqaacnd100% (1)
- Study of Pattern of Acute Myocardial Infarction in Tertiary Care Hospital of Ahmedabad, GujaratDocument6 pagesStudy of Pattern of Acute Myocardial Infarction in Tertiary Care Hospital of Ahmedabad, GujaratEditor_IAIMNo ratings yet
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Document4 pagesAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiNo ratings yet
- EjpmrDocument7 pagesEjpmrSrikanth SriramaNo ratings yet
- C Reaktive ProteinDocument4 pagesC Reaktive Proteinsinggih2008No ratings yet
- Articol Rev Med Chirrefacut OvidiuDocument8 pagesArticol Rev Med Chirrefacut OvidiuNicu IacobNo ratings yet
- The Type of The Functional Cardiovascular Response To Upright Posture Is Associated With Arterial Stiffness: A Cross-Sectional Study in 470 VolunteersDocument12 pagesThe Type of The Functional Cardiovascular Response To Upright Posture Is Associated With Arterial Stiffness: A Cross-Sectional Study in 470 VolunteersVeNo ratings yet
- Plasma Concentration of C-Reactive Protein and Risk of Developing Peripheral Vascular DiseaseDocument8 pagesPlasma Concentration of C-Reactive Protein and Risk of Developing Peripheral Vascular Diseaseashphoenix32No ratings yet
- Jurnal 5Document6 pagesJurnal 5Siti rahmi AbukhaerNo ratings yet
- Caufriez J Clin Endocrinol Metab 2021 SR Progesterone On SleepDocument2 pagesCaufriez J Clin Endocrinol Metab 2021 SR Progesterone On SleepPaul PIETTENo ratings yet
- NAMS 2022 Hormone-Therapy-Position-StatementDocument28 pagesNAMS 2022 Hormone-Therapy-Position-StatementPaul PIETTENo ratings yet
- Piette Climacteric 2018 The History of Natural Progesterone The Never Ending StoryDocument8 pagesPiette Climacteric 2018 The History of Natural Progesterone The Never Ending StoryPaul PIETTENo ratings yet
- Piette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteroneDocument17 pagesPiette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteronePaul PIETTENo ratings yet
- Mononobe OkabeDocument11 pagesMononobe Okabe24x7civilconsultantNo ratings yet
- HRM Issues and Challenges in Cooperative Banks in IndiaDocument6 pagesHRM Issues and Challenges in Cooperative Banks in Indiaghanshamdas67% (3)
- Curriculum Vitae - Dr. Antonis LiakosDocument3 pagesCurriculum Vitae - Dr. Antonis LiakosCanadaUsaNetNo ratings yet
- L1 - Methods of Tissue Examination & Preparation and Tissue SamplingDocument47 pagesL1 - Methods of Tissue Examination & Preparation and Tissue SamplingsademNo ratings yet
- Gods Revelation in Jesus and in His ChurchDocument13 pagesGods Revelation in Jesus and in His ChurchMerry DaceraNo ratings yet
- Merchant Banking Roles and FunctionsDocument18 pagesMerchant Banking Roles and Functionssunita prabhakarNo ratings yet
- Mock Exam Practice - ListeningDocument5 pagesMock Exam Practice - ListeningChristeen221No ratings yet
- Scada/Ems/Dms: Electric Utilities Networks & MarketsDocument12 pagesScada/Ems/Dms: Electric Utilities Networks & MarketsdoquocdangNo ratings yet
- Philippines Supreme Court rules on robbery and double homicide caseDocument13 pagesPhilippines Supreme Court rules on robbery and double homicide caseNadzlah BandilaNo ratings yet
- Critical Book Review Seminar on ELTDocument4 pagesCritical Book Review Seminar on ELTLiza GunawanNo ratings yet
- Google App Engine: A Platform for Developing and Hosting Web AppsDocument5 pagesGoogle App Engine: A Platform for Developing and Hosting Web AppsnagrajNo ratings yet
- Assignment Fundamentals of Book - Keeping & AccountingDocument19 pagesAssignment Fundamentals of Book - Keeping & AccountingmailonvikasNo ratings yet
- Digital Image Processing: Relationships of PixelDocument49 pagesDigital Image Processing: Relationships of PixelAiNo ratings yet
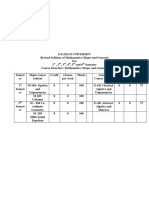
- TDC - Syllabus Mathematics PDFDocument32 pagesTDC - Syllabus Mathematics PDFAnanta PaulNo ratings yet
- Mechatronics Definition:: Task 1 - P1Document7 pagesMechatronics Definition:: Task 1 - P1mrssahar100% (1)
- Directions To Candidates Paper 1 - MedicalDocument29 pagesDirections To Candidates Paper 1 - MedicalMedicEdNo ratings yet
- The Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsDocument7 pagesThe Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsMuthu BaskaranNo ratings yet
- Reaction KineticsDocument37 pagesReaction KineticsDaisyNo ratings yet
- 5th Grade 13-14 Math Common Core Standards by QuarterDocument3 pages5th Grade 13-14 Math Common Core Standards by QuartermrkballNo ratings yet
- Nuisance or Natural and Healthy Should Monthly Menstruation Be Optional For Women PDFDocument3 pagesNuisance or Natural and Healthy Should Monthly Menstruation Be Optional For Women PDFDieWeisseLeserinNo ratings yet
- Kombai DogsDocument5 pagesKombai Dogschandan.belagundaNo ratings yet
- The Nightingale and The RoseDocument23 pagesThe Nightingale and The RosesaimaNo ratings yet
- Paper 6D - Appeals & Days Time Limits (By Khader)Document6 pagesPaper 6D - Appeals & Days Time Limits (By Khader)Khader MohammedNo ratings yet
- Pem735 D00084 D XxenDocument6 pagesPem735 D00084 D XxenYigit SarıkayaNo ratings yet