You might also like
- PADIS Guidelines Teaching Slides PainDocument43 pagesPADIS Guidelines Teaching Slides Pain陳政吉No ratings yet
- Rapid Diagnostic Tests For Covid-19Document4 pagesRapid Diagnostic Tests For Covid-19Febri RirinNo ratings yet
- Akash Covid ReportDocument1 pageAkash Covid ReportGenestrings Diagnostic CenterNo ratings yet
- Critical Appraisal of The TopicsDocument13 pagesCritical Appraisal of The TopicsRyan AndhikaNo ratings yet
- Cat Uro Fenis ErecioDocument13 pagesCat Uro Fenis Erecioahmad iffa maududyNo ratings yet
- DRUG+STUDY NaprexDocument2 pagesDRUG+STUDY NaprexJoevence Gazo CuaresmaNo ratings yet
- Critical Appraisal of The TopicsDocument13 pagesCritical Appraisal of The TopicsIntan Eklesiana NapitupuluNo ratings yet
- Sepsis AlgorithmDocument1 pageSepsis AlgorithmAshly Nygil100% (1)
- 7 Cases FungalDocument56 pages7 Cases Fungalkoteshwara raoNo ratings yet
- Acute Gastroenteritis Nelsons CHPDocument48 pagesAcute Gastroenteritis Nelsons CHPd99452727No ratings yet
- COVID TEST ALGORITHM (Wef: April 10, 2021) : Also CalledDocument3 pagesCOVID TEST ALGORITHM (Wef: April 10, 2021) : Also CalledArun MathewNo ratings yet
- 5 Cases FungalDocument56 pages5 Cases Fungalkoteshwara raoNo ratings yet
- Drug StudyDocument2 pagesDrug StudyMarie Ashley CasiaNo ratings yet
- QPCM, Specimen Collection Guide, Mount Sinai, GovDocument74 pagesQPCM, Specimen Collection Guide, Mount Sinai, GovFilipus HendiantoNo ratings yet
- Wa0001.Document2 pagesWa0001.akashcool470No ratings yet
- Communicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Document11 pagesCommunicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Casilda FranciscoNo ratings yet
- Pediatric Community Acquired PneumoniaDocument4 pagesPediatric Community Acquired PneumoniaEspie FerrerNo ratings yet
- Blood Test - LFTDocument4 pagesBlood Test - LFTAbhi NikamNo ratings yet
- Covid 19 Testing Overview Molecular Antigen Antibody 0920Document2 pagesCovid 19 Testing Overview Molecular Antigen Antibody 0920ArdityaNo ratings yet
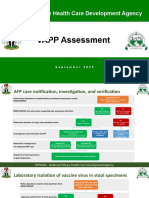
- VAPP Job AidDocument5 pagesVAPP Job AidTella AdedamolaNo ratings yet
- Orthopaedic Infection in Adults UHL GuidelineDocument10 pagesOrthopaedic Infection in Adults UHL GuidelineFadlu ManafNo ratings yet
- ScopeDocument11 pagesScopemosmarNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument6 pagesNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale Evaluationamebernardo88No ratings yet
- Laboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesDocument20 pagesLaboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesYayax RakhmanNo ratings yet
- Covid-19 Test Report: Patient Name: Gurvinder AroraDocument1 pageCovid-19 Test Report: Patient Name: Gurvinder AroraGenestrings Diagnostic CenterNo ratings yet
- Fast Results 15 Minutes Assay Time Easy Visuallly Interpretation Simple Operation, No Equipment Required High AccuracyDocument1 pageFast Results 15 Minutes Assay Time Easy Visuallly Interpretation Simple Operation, No Equipment Required High AccuracyIbnu Abdul AzizNo ratings yet
- MRSA Contact Precautions Removal Algorithm: Are Either of The Boxes Checked?Document1 pageMRSA Contact Precautions Removal Algorithm: Are Either of The Boxes Checked?bayu bayuNo ratings yet
- False Negative Tests For SARS-CoV-2 Infection - Challenges and ImplicationDocument3 pagesFalse Negative Tests For SARS-CoV-2 Infection - Challenges and ImplicationsamuelNo ratings yet
- Quinto, Gemma (NCP & DRUG STUDY)Document13 pagesQuinto, Gemma (NCP & DRUG STUDY)Mariam Yiani Aspiras RacelesNo ratings yet
- Critical Appraisal of The TopicsDocument10 pagesCritical Appraisal of The TopicsRupita SitanggangNo ratings yet
- 10 1097@aog 0000000000003857Document2 pages10 1097@aog 0000000000003857Manuel MagañaNo ratings yet
- Covid-19 Test Report: PATIENT NAME: Indu Gupta Raj BalaDocument1 pageCovid-19 Test Report: PATIENT NAME: Indu Gupta Raj BalaTarun BhatnagarNo ratings yet
- Villamaria - Drug StudyDocument11 pagesVillamaria - Drug StudyHey LeunNo ratings yet
- CAT Onko - Adhitya Wisnu MahadewaDocument9 pagesCAT Onko - Adhitya Wisnu Mahadewaahmad iffa maududyNo ratings yet
- Endo 5Document1 pageEndo 5Bea YmsnNo ratings yet
- Immunological, Viral and Genetic Basis of COVID-19 in Local Patients (RRG # 211)Document38 pagesImmunological, Viral and Genetic Basis of COVID-19 in Local Patients (RRG # 211)محمد بلال سرورNo ratings yet
- Presentation2 (Auto-Saved) 2Document38 pagesPresentation2 (Auto-Saved) 2محمد بلال سرورNo ratings yet
- Loop-Mediated Isothermal Amplification Test For The Molecular Diagnosis of MalariaDocument14 pagesLoop-Mediated Isothermal Amplification Test For The Molecular Diagnosis of MalariahgchgNo ratings yet
- Development and Validation of A Scoring System For DifferentDocument7 pagesDevelopment and Validation of A Scoring System For DifferentmadhumidhaNo ratings yet
- Cat AvfDocument11 pagesCat AvfS3V4_9154No ratings yet
- Intestinal ParasitesDocument1 pageIntestinal ParasitesSabir YeddiNo ratings yet
- Part 2 210-273Document64 pagesPart 2 210-273alrabaee92No ratings yet
- 10 1001@jama 2020 8259 PDFDocument3 pages10 1001@jama 2020 8259 PDFTriLightNo ratings yet
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicineNguyễn HàNo ratings yet
- CAT Bedah VaskularDocument10 pagesCAT Bedah Vaskulardikiprestya391No ratings yet
- Day 2 TB Diagnostics - MacalaladDocument45 pagesDay 2 TB Diagnostics - MacalaladRye CalderonNo ratings yet
- STEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsDocument2 pagesSTEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsahjkseflhasefNo ratings yet
- Diagnostic TestsDocument5 pagesDiagnostic TestsAastha jainNo ratings yet
- Studies Summary in OphthalmologyDocument12 pagesStudies Summary in OphthalmologyMuhammad Usman Ghani GormaniNo ratings yet
- CAT Jurnal Ortho IfaDocument10 pagesCAT Jurnal Ortho Ifaahmad iffa maududyNo ratings yet
- Adult Syphilis Staging, Treatment and Partner ManagementDocument4 pagesAdult Syphilis Staging, Treatment and Partner ManagementchandanNo ratings yet
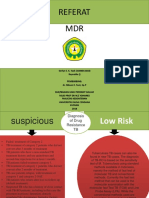
- MDR ReferatDocument12 pagesMDR ReferatIntan Princess SweetNo ratings yet
- Algorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Document1 pageAlgorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Ashton KryzanowskiNo ratings yet
- Algorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Document1 pageAlgorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Het NandaaanaNo ratings yet
- ReportDocument1 pageReportDhruv RanaNo ratings yet
- Near-Infrared-Based Cerebral Oximetry For Prediction of Severe Acute Kidney InjuryDocument9 pagesNear-Infrared-Based Cerebral Oximetry For Prediction of Severe Acute Kidney InjuryOğuz KayıkçıNo ratings yet
- Mindray CLIA - SARS-CoV-2 IgM and IgG (June 2020)Document7 pagesMindray CLIA - SARS-CoV-2 IgM and IgG (June 2020)enzaeniNo ratings yet
- CAT - Kelompok 1Document8 pagesCAT - Kelompok 1AndikaChandraNo ratings yet
- 1st DayDocument3 pages1st DayLyrechel de GuzmanNo ratings yet
- Textbook of in vivo Imaging in VertebratesFrom EverandTextbook of in vivo Imaging in VertebratesVasilis NtziachristosNo ratings yet
- Surgery in General Residency Training Requirements (As at 20 Oct 21)Document15 pagesSurgery in General Residency Training Requirements (As at 20 Oct 21)Jawariya ZiaNo ratings yet
- Neurosurgery Residency Training Requirements (Revised Approv 20 July 22)Document11 pagesNeurosurgery Residency Training Requirements (Revised Approv 20 July 22)Jawariya ZiaNo ratings yet
- Job AdvertisementDocument7 pagesJob AdvertisementJawariya ZiaNo ratings yet
- Antimicrobial Prophylaxis in Total Hip Replacement: A Systematic ReviewDocument67 pagesAntimicrobial Prophylaxis in Total Hip Replacement: A Systematic ReviewJawariya ZiaNo ratings yet
- Splenectomy in Sickle Cell Anemia: of A Case and Review of The LiteratureDocument7 pagesSplenectomy in Sickle Cell Anemia: of A Case and Review of The LiteratureJawariya ZiaNo ratings yet
- 2020MyPlatePlan 2000cals Age14+Document2 pages2020MyPlatePlan 2000cals Age14+Jawariya ZiaNo ratings yet
- Your Spinal AnaestheticDocument7 pagesYour Spinal AnaestheticJawariya ZiaNo ratings yet
- User Manual PRPDocument12 pagesUser Manual PRPJawariya ZiaNo ratings yet
- Immunology: TEST(s) Normal UNIT(s)Document1 pageImmunology: TEST(s) Normal UNIT(s)Jawariya ZiaNo ratings yet
- Supplements UPDATED - OCT 2023Document9 pagesSupplements UPDATED - OCT 2023r_sendhilNo ratings yet
- 13 Chapter 5Document64 pages13 Chapter 5yoganaNo ratings yet
- Amisulpride Tablets I.P.: 50mg, 100mg, 200mg and 400 MGDocument7 pagesAmisulpride Tablets I.P.: 50mg, 100mg, 200mg and 400 MGJoon SiangNo ratings yet
- Nama ObatDocument13 pagesNama Obatsahmin sahminNo ratings yet
- Daftar Kebutuhan Obat 2021 (Emergency)Document6 pagesDaftar Kebutuhan Obat 2021 (Emergency)dini mahdianiNo ratings yet
- Introduction STGDocument2 pagesIntroduction STGdineshmarginalNo ratings yet
- YFT IM Notes 2Document81 pagesYFT IM Notes 2AHMAD ALROWAILYNo ratings yet
- Acute Coronary Syndrome - AMBOSSDocument31 pagesAcute Coronary Syndrome - AMBOSSSarah Ronquillo100% (1)
- Potential Antiinfluenza Effective Plants Used in Turkish Folk Medicine A Review2021journal of EthnopharmacologyDocument22 pagesPotential Antiinfluenza Effective Plants Used in Turkish Folk Medicine A Review2021journal of EthnopharmacologySucowatiNo ratings yet
- Protocol For Treatment of Anaphylactic ReactionsDocument1 pageProtocol For Treatment of Anaphylactic ReactionsbuenaNo ratings yet
- What Is Treatment of Hypertension?Document11 pagesWhat Is Treatment of Hypertension?health usefulNo ratings yet
- Formulation and Evaluation of Levodropropizine LozengesDocument14 pagesFormulation and Evaluation of Levodropropizine LozengesFitria MokodompitNo ratings yet
- VPH0072 - Analyzing Cannabis Flowers According To The German Pharmacopeia - Monograph 2018Document4 pagesVPH0072 - Analyzing Cannabis Flowers According To The German Pharmacopeia - Monograph 2018qa managerNo ratings yet
- May Recall 2021Document47 pagesMay Recall 2021school adressNo ratings yet
- B. Hormones, General Principles by D SiwaleDocument73 pagesB. Hormones, General Principles by D SiwaleDonald SiwaleNo ratings yet
- Introduction To Nursing PharmacologyDocument7 pagesIntroduction To Nursing Pharmacologyastraeax pandaNo ratings yet
- Hypothyroidism in Context: Where We've Been and Where We're GoingDocument12 pagesHypothyroidism in Context: Where We've Been and Where We're Going1130017003 AIMMATUL CHANIFAHNo ratings yet
- Important Notice 38-2021 Dated 24-03-2021 Available Seats Foreign National Spon INI CET PG Courses July 2021Document3 pagesImportant Notice 38-2021 Dated 24-03-2021 Available Seats Foreign National Spon INI CET PG Courses July 2021Priyobrata KonjengbamNo ratings yet
- PowerPoint AntidepressantsDocument29 pagesPowerPoint AntidepressantsRaeika GanjiNo ratings yet
- Ganoderma MechanismDocument12 pagesGanoderma MechanismJorge Luis Plasencia CubaNo ratings yet
- 606 Ccaf 8Document3 pages606 Ccaf 8Nisha RajiNo ratings yet
- ZAHID MEHMOOD CVDocument4 pagesZAHID MEHMOOD CVMadiha MahfoozNo ratings yet
- Pharmacotherapeutics in ObstetricsDocument103 pagesPharmacotherapeutics in Obstetricssanthanalakshmi100% (4)
- Multiple Choice Questions: Enhanced Recovery For Lower Limb ArthroplastyDocument5 pagesMultiple Choice Questions: Enhanced Recovery For Lower Limb ArthroplastyMaid LampardNo ratings yet
- Company Profile Incepta PharmaDocument9 pagesCompany Profile Incepta PharmaNobo AhmedNo ratings yet
- An Overview of Asthma Management - UpToDateDocument31 pagesAn Overview of Asthma Management - UpToDateSantiago Mondragon RiosNo ratings yet
- Breastfeeding: PregnancyDocument40 pagesBreastfeeding: PregnancyCelestial DawnNo ratings yet
- Reverse Pharmacological Correlates of Ayurvedic DRDocument6 pagesReverse Pharmacological Correlates of Ayurvedic DRCiontu ValentinNo ratings yet
- Acetaminophen Toxicity in ChildrenDocument5 pagesAcetaminophen Toxicity in Childrendaniascl9527No ratings yet