You might also like
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- Caring For The Mechanically Ventilated PatientDocument2 pagesCaring For The Mechanically Ventilated PatientKat AlaNo ratings yet
- Contin Educ Anaesth Crit Care Pain-2005-Lermitte-113-7Document5 pagesContin Educ Anaesth Crit Care Pain-2005-Lermitte-113-7pediatria hncaseNo ratings yet
- NCP Impaired Gas ExchangeDocument2 pagesNCP Impaired Gas ExchangeCharissa Magistrado De LeonNo ratings yet
- Requirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaDocument7 pagesRequirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaChloie Marie RosalejosNo ratings yet
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaLeogalvez BedanoNo ratings yet
- Asthma AssessmentDocument1 pageAsthma AssessmentnarstinesirkNo ratings yet
- Cecilia, Issaiah Nicolle-Pneumothorax-NcpDocument7 pagesCecilia, Issaiah Nicolle-Pneumothorax-NcpIssaiah Nicolle Cecilia100% (1)
- Mechanical VentilatorDocument2 pagesMechanical VentilatorNat MarzanNo ratings yet
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancepeter_degamo20000% (1)
- AssessmentDocument1 pageAssessmentFat NrqzNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- Impaire Spontaneous VentilationDocument4 pagesImpaire Spontaneous VentilationSkyla FiestaNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanRenea Joy ArruejoNo ratings yet
- NUR 103A RLE Learning Activity - PneumothoraxDocument8 pagesNUR 103A RLE Learning Activity - PneumothoraxLaica & AivanNo ratings yet
- Clinical Teaching On Ventilator Settings and ModeDocument21 pagesClinical Teaching On Ventilator Settings and Modejyoti punia100% (1)
- Mechanical Ventilator HandoutsDocument4 pagesMechanical Ventilator HandoutsDarwin AndalNo ratings yet
- St. Anthony's Nursing Care PlanDocument2 pagesSt. Anthony's Nursing Care PlanKristine Young100% (1)
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- NCP Near DrowningDocument1 pageNCP Near Drowningchristine louise bernardoNo ratings yet
- Mechanical Ventilation Mechanical Ventilation: Dr. Ravi Gadani MS, Fmas Dr. Ravi Gadani MS, FmasDocument35 pagesMechanical Ventilation Mechanical Ventilation: Dr. Ravi Gadani MS, Fmas Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- ChurvaDocument103 pagesChurvachabot871No ratings yet
- ACUTE RESPIRATORY DISTRESSDocument1 pageACUTE RESPIRATORY DISTRESSchristine louise bernardo100% (1)
- NCPDocument3 pagesNCPMichael TokongNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- Nursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaDocument5 pagesNursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaSofiaLopezNo ratings yet
- ANAPHYLAXIS CAREDocument6 pagesANAPHYLAXIS CAREKirstin del CarmenNo ratings yet
- Mechanical VentilationDocument16 pagesMechanical VentilationBhawna JoshiNo ratings yet
- N Engl J Med 2022 387 1688 - AppendixDocument6 pagesN Engl J Med 2022 387 1688 - AppendixAdriana MartinezNo ratings yet
- Nursing Care Plan For Ineffective Airway ClearanceDocument6 pagesNursing Care Plan For Ineffective Airway ClearanceCaroline ChaNo ratings yet
- AssessmentDocument7 pagesAssessmentSheryhan Tahir BayleNo ratings yet
- Unit III (C) Ventilator CareDocument20 pagesUnit III (C) Ventilator CarePriya bhattiNo ratings yet
- Airway & Ventilatory Management1Document7 pagesAirway & Ventilatory Management1anon-623422100% (1)
- Cues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationNichol John MalabananNo ratings yet
- NCPPDocument11 pagesNCPPAngelo Miguel MuñozNo ratings yet
- Airway Control and Ventilation TechniquesDocument33 pagesAirway Control and Ventilation TechniquespercivicNo ratings yet
- FOT INGLESDocument3 pagesFOT INGLESdicova43No ratings yet
- General Principles of Mechanical VentilationDocument21 pagesGeneral Principles of Mechanical VentilationCarlos UrquijoNo ratings yet
- Ventilatory Support in The Intensive Care UnitDocument8 pagesVentilatory Support in The Intensive Care UnitDamian AriasNo ratings yet
- Critical Care Clinical Procedures 2023Document38 pagesCritical Care Clinical Procedures 2023nucahersheyskatNo ratings yet
- Nursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBDocument24 pagesNursing Care Plan Client: N. D. Age: 39 Gender: Male Medical Diagnosis: Community Acquired Pneumonia, Moderate Risk, PTBGertrude Araneta JavierNo ratings yet
- NCP NRMFDocument2 pagesNCP NRMFJai CortezNo ratings yet
- 43 Adaptive Support Ventilation As VDocument5 pages43 Adaptive Support Ventilation As Vnanang criztaNo ratings yet
- Provide assistancein activities of dailyliving as needed toconserve energy forrespirationDocument6 pagesProvide assistancein activities of dailyliving as needed toconserve energy forrespirationCuttie Anne GalangNo ratings yet
- Nursi NG Care Plan: Cues Nursing Diagnosis Planning Nursing Intervention Rationale Expected OutcomeDocument2 pagesNursi NG Care Plan: Cues Nursing Diagnosis Planning Nursing Intervention Rationale Expected OutcomeErika Mae MananganNo ratings yet
- ASSESSMENTDocument2 pagesASSESSMENTArvin BaesNo ratings yet
- Care of Patient On VentilatorDocument18 pagesCare of Patient On VentilatorJose Paul Rader100% (1)
- Mechanical Ventilator: Parameters of Mechanical VentilationDocument7 pagesMechanical Ventilator: Parameters of Mechanical Ventilationpraveen joseNo ratings yet
- Bautista - 3 Way Bottle SystemDocument4 pagesBautista - 3 Way Bottle SystemKatherine BautistaNo ratings yet
- Nursing Care Plan for COPD Patient's OxygenationDocument3 pagesNursing Care Plan for COPD Patient's OxygenationMiar QuestNo ratings yet
- NURSING INTERVENTIONS FOR INEFFECTIVE BREATHING PATTERNDocument7 pagesNURSING INTERVENTIONS FOR INEFFECTIVE BREATHING PATTERNDanica Kate GalleonNo ratings yet
- 4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)Document5 pages4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)SONY MANDAPNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationGiddel Guerra PapellerasNo ratings yet
- Final-Intubation Extubation Plus (1) - 1Document112 pagesFinal-Intubation Extubation Plus (1) - 1Lylibette Anne CalimlimNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- Fundamentals of Nursing TheoriesDocument78 pagesFundamentals of Nursing TheoriesLovely Cervantes100% (1)
- Cranial Nerve ChartDocument1 pageCranial Nerve Chartルフィ モンキー り50% (2)
- Republic Act No. 10912 "Continuing Professional Development (CPD) Act of 2016"Document3 pagesRepublic Act No. 10912 "Continuing Professional Development (CPD) Act of 2016"Lovely CervantesNo ratings yet
- PharmacologyDocument10 pagesPharmacologyPrince Mark Badillo100% (2)
- Congenital Disorders of The Skeletal SystemDocument64 pagesCongenital Disorders of The Skeletal SystemLovely CervantesNo ratings yet
- Parkinsons DiseaseDocument37 pagesParkinsons DiseaseLovely CervantesNo ratings yet
- BP Regulation Medications: MOA, Adverse Effects, Clinical ConsiderationsDocument5 pagesBP Regulation Medications: MOA, Adverse Effects, Clinical ConsiderationsLovely CervantesNo ratings yet
- Myasthenia GravisDocument33 pagesMyasthenia GravisLovely Cervantes100% (1)
- Common Emergency DrugsDocument1 pageCommon Emergency DrugsFreeNursingNotesNo ratings yet
- Ineffective Breathing PatternDocument5 pagesIneffective Breathing PatternruguNo ratings yet
- Texas Children's Center For Telehealth Nursing and Allied Health Professionals Distance Education and CNE/CEU OfferingDocument35 pagesTexas Children's Center For Telehealth Nursing and Allied Health Professionals Distance Education and CNE/CEU Offeringabdo_hegaze100% (1)
- Respiratory System Assessment PDFDocument53 pagesRespiratory System Assessment PDFJay RomeNo ratings yet
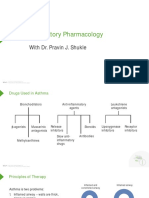
- Respiratory Pharmacology: With Dr. Pravin J. ShukleDocument28 pagesRespiratory Pharmacology: With Dr. Pravin J. ShukleKaish DahiyaNo ratings yet
- Protocol For Heart Rate Variability Biofeedback TrainingDocument13 pagesProtocol For Heart Rate Variability Biofeedback TrainingLevente BalázsNo ratings yet
- Ta 8Document4 pagesTa 8thanh nganNo ratings yet
- Asuhan Kefarmasian Pada Pasien Asma Dan PPOKDocument61 pagesAsuhan Kefarmasian Pada Pasien Asma Dan PPOKAni SetiyawatiNo ratings yet
- Asthma Small Group DiscussionDocument12 pagesAsthma Small Group DiscussionLyca Mae AurelioNo ratings yet
- AsthmaDocument57 pagesAsthmaVladanNo ratings yet
- Respiration in organisms explainedDocument17 pagesRespiration in organisms explainedDrRudresh SajjanNo ratings yet
- Capnograpy Ems Waveform Reference CardDocument2 pagesCapnograpy Ems Waveform Reference CardMayHnin Khaing100% (1)
- Lung Disease and Copd Seminar PresentationDocument14 pagesLung Disease and Copd Seminar Presentationapi-402325622No ratings yet
- Case Study On AsthmaDocument18 pagesCase Study On AsthmaFritzielove BayawaNo ratings yet
- Mind Map - Respiratory SystemDocument1 pageMind Map - Respiratory SystemHaziraAzlyNo ratings yet
- Sodium Dichromate MSDSDocument6 pagesSodium Dichromate MSDShamMhamNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Sotfonic SotfonicNo ratings yet
- Nursing Diagnosis PneumoniaDocument1 pageNursing Diagnosis PneumoniaPasa ShresthaNo ratings yet
- Bronchial AsthmaDocument10 pagesBronchial AsthmaHlaSoe WinNo ratings yet
- AEA - Ambulance Emergency Assistant - ProtocolsDocument12 pagesAEA - Ambulance Emergency Assistant - ProtocolsM Gavin100% (4)
- Chestgra、 Ph Hl-101: Spirometry SystemDocument2 pagesChestgra、 Ph Hl-101: Spirometry SystemDiep NguyentuanNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanAnthea ValinoNo ratings yet
- CS4 Asthma Drug StudyDocument10 pagesCS4 Asthma Drug StudyAudrie Allyson GabalesNo ratings yet
- ST John Ambulance 2020 (Choking)Document11 pagesST John Ambulance 2020 (Choking)Praveena MoganNo ratings yet
- Anatomy - RespirationDocument2 pagesAnatomy - RespirationpherociousNo ratings yet
- Clinical Examination of Respiratory SystemDocument37 pagesClinical Examination of Respiratory SystemDipienshu BhatNo ratings yet
- Lec 38drugs Used in AsthmaDocument19 pagesLec 38drugs Used in AsthmaAbdul MananNo ratings yet
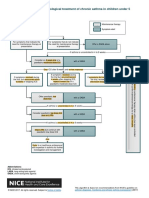
- Algorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5Document1 pageAlgorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5samNo ratings yet
- Dupilumab Improves Upper and Lower Airway Disease Control in Chronic Rhinosinusitis With Nasal Polyps and AsthmaDocument10 pagesDupilumab Improves Upper and Lower Airway Disease Control in Chronic Rhinosinusitis With Nasal Polyps and AsthmaMeylinda RizkyNo ratings yet
- 3 3 1 Medical History Visit 1Document2 pages3 3 1 Medical History Visit 1api-32993253456% (9)
- 4 - Asthma Dan Status AsthmaticusDocument49 pages4 - Asthma Dan Status AsthmaticusMaspupah Widiyanti RachmatNo ratings yet