You might also like
- Oktawati 2020Document3 pagesOktawati 2020Mariatun ZahronasutionNo ratings yet
- Junral 1Document5 pagesJunral 1Metta WinniNo ratings yet
- Case Studies Collection 22Document39 pagesCase Studies Collection 22Eduard ConstantinNo ratings yet
- Idjsr Se 0168Document4 pagesIdjsr Se 0168Alfan MaulanaNo ratings yet
- Lasers in Endodontics ReviewDocument7 pagesLasers in Endodontics ReviewKalpanaNo ratings yet
- Aumento de Papila Interdental Con PRF 3Document6 pagesAumento de Papila Interdental Con PRF 3Francisco Javier Mardones QuintanillaNo ratings yet
- PolypExcision EJBPS 2015 PDFDocument9 pagesPolypExcision EJBPS 2015 PDFdeespepeNo ratings yet
- JInterdiscipDentistry12119-4138785 112947 PDFDocument6 pagesJInterdiscipDentistry12119-4138785 112947 PDFAndamiaNo ratings yet
- Beak and Bumper - Physics Forceps: Evaluation of New Technique in ExtractionDocument10 pagesBeak and Bumper - Physics Forceps: Evaluation of New Technique in ExtractionWuppuluri Jayanth Kumar SharmaNo ratings yet
- Dentistry Oraldisorders Therapy30Document6 pagesDentistry Oraldisorders Therapy30muhammadNo ratings yet
- Do Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."Document5 pagesDo Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."arshad khandayNo ratings yet
- Case Report Endo Perio Lesions-A Synergistic ApproachDocument5 pagesCase Report Endo Perio Lesions-A Synergistic ApproachRyanka Dizayani PutraNo ratings yet
- ARTUCULO DR CHAVEZ AMELOGENESIS13256 - 2020 - Article - 2586Document7 pagesARTUCULO DR CHAVEZ AMELOGENESIS13256 - 2020 - Article - 2586marcelaNo ratings yet
- Comparative Evaluation of Marginal Integrity of GlassDocument7 pagesComparative Evaluation of Marginal Integrity of Glassbodas de plata Odontologia UNFVNo ratings yet
- Deep Margin Elevation For Indirect Restorations: A Systematic ReviewDocument9 pagesDeep Margin Elevation For Indirect Restorations: A Systematic ReviewIvy MedNo ratings yet
- Putra,+56 Bmj.v9i1.1668Document6 pagesPutra,+56 Bmj.v9i1.1668Ilham Nugraha SyahputraNo ratings yet
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 pagesNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNo ratings yet
- Splinting Case ReportDocument5 pagesSplinting Case Report0030-GRETANZA HENDRAT MONICANo ratings yet
- Effect of Low Level Laser Therapy On Wound Healing AfterDocument6 pagesEffect of Low Level Laser Therapy On Wound Healing AfterYou're Just As Sane As DivaNo ratings yet
- pg70-71 Periodontal ManagementDocument2 pagespg70-71 Periodontal ManagementJackie CooperNo ratings yet
- Wjo 11 4 Gandedkar 9Document12 pagesWjo 11 4 Gandedkar 9Vijay ChinthaNo ratings yet
- Informe Endo 2Document7 pagesInforme Endo 2Angel LampreaNo ratings yet
- 1.1 Comparison Between Integrated and Parallel Interlock Designs of An Extracoronal Attachment-Retained Distal Extension Removable Partial DenturesDocument9 pages1.1 Comparison Between Integrated and Parallel Interlock Designs of An Extracoronal Attachment-Retained Distal Extension Removable Partial DenturesOaNa GrigorutaNo ratings yet
- Ledermix Pulp Treatment in A Permanent Molar A CasDocument8 pagesLedermix Pulp Treatment in A Permanent Molar A Casqiao fenNo ratings yet
- Regenerative Endodontics-Potential Approaches in Revitalizing The Tooth Pulp - A Review ArticleDocument7 pagesRegenerative Endodontics-Potential Approaches in Revitalizing The Tooth Pulp - A Review ArticleMelliya heptaniaNo ratings yet
- JPharmBioallSci95295-3690707 101507Document4 pagesJPharmBioallSci95295-3690707 101507ayoubNo ratings yet
- Apiko 1Document5 pagesApiko 1Asri DamayantiNo ratings yet
- Photobio-Root ResorptionDocument9 pagesPhotobio-Root Resorptionhassankhan9849No ratings yet
- Apical Limit 2009Document7 pagesApical Limit 2009wanda oktariaNo ratings yet
- Frenectomy As A Multidisciplinary Prostho-Perio Management Approach For Partial Denture-A Case ReportDocument6 pagesFrenectomy As A Multidisciplinary Prostho-Perio Management Approach For Partial Denture-A Case ReportMidda SosmedNo ratings yet
- Periodontal Accelerated Osteogenic Orthodontics Technique For RapidDocument10 pagesPeriodontal Accelerated Osteogenic Orthodontics Technique For RapidATZIRI CHAVEZ PORTILLONo ratings yet
- Protesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarDocument13 pagesProtesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarAngela AcostaNo ratings yet
- Relationship_between_Deep_MargDocument10 pagesRelationship_between_Deep_Margcd.brendasotofloresNo ratings yet
- ArticulosDocument7 pagesArticuloslupita.sm1988No ratings yet
- Jurnal Resesi Gingiva 2Document7 pagesJurnal Resesi Gingiva 2Muhammad KholisNo ratings yet
- Clinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportDocument6 pagesClinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportIqra KhanNo ratings yet
- Gingival_displacement_for_impression_making_in_fixDocument26 pagesGingival_displacement_for_impression_making_in_fixSushmaNo ratings yet
- 23 Case Rep1 Palatogingival GrooveDocument7 pages23 Case Rep1 Palatogingival GrooveDr.O.R.GANESAMURTHINo ratings yet
- Tanpa Judul PDFDocument3 pagesTanpa Judul PDFnadyashintakasihNo ratings yet
- DR Bhaumik Nanavati Proof ApprovedDocument6 pagesDR Bhaumik Nanavati Proof ApprovedFahmi FirmansyahNo ratings yet
- Management of The Open Apex Using New Biomaterials: 10.5005/jp-Journals-10047-0055Document5 pagesManagement of The Open Apex Using New Biomaterials: 10.5005/jp-Journals-10047-0055Asmita SonawneNo ratings yet
- Ex Vivo Microbial Leakage Analysis of Polytetrafluoroethylene Tape and Cotton Pellet As Endodontic Access Cavity SpacersDocument7 pagesEx Vivo Microbial Leakage Analysis of Polytetrafluoroethylene Tape and Cotton Pellet As Endodontic Access Cavity SpacersAbhishek Isaac MathewNo ratings yet
- Apicoectomy of Palatal Root in Upper 1 Molar To Remove Endodontic Instrument: Rare Case ReportDocument4 pagesApicoectomy of Palatal Root in Upper 1 Molar To Remove Endodontic Instrument: Rare Case ReportUmarsyah AliNo ratings yet
- 7 TH JC PDF - SindhuDocument5 pages7 TH JC PDF - SindhuDadi SindhuNo ratings yet
- Endodontic ArmamentariumDocument29 pagesEndodontic ArmamentariumAbdulSamiNo ratings yet
- 33 RD JC - SoniaDocument9 pages33 RD JC - SoniaDadi SindhuNo ratings yet
- Endodontology31168-7965184 220731Document4 pagesEndodontology31168-7965184 220731Asmita SonawneNo ratings yet
- Recent Advances in Endodontics Ndash A Perspective ReviewDocument4 pagesRecent Advances in Endodontics Ndash A Perspective ReviewMaría de la Caridad BarcielaNo ratings yet
- Perceptions of NZ Orthodontists and Periodontists On The Management of Gingival Recession in Orthodontic PatientsDocument10 pagesPerceptions of NZ Orthodontists and Periodontists On The Management of Gingival Recession in Orthodontic PatientsSenussi IbtisamNo ratings yet
- Retramiento Cami 5Document5 pagesRetramiento Cami 5Jorge GuetteNo ratings yet
- Journal Laser and Its Use in Pediatric Dentistry A ReviewDocument5 pagesJournal Laser and Its Use in Pediatric Dentistry A ReviewTiaraNo ratings yet
- Laser and Its Use in Pediatric Dentistry: A Review of Literature and A Recent UpdateDocument5 pagesLaser and Its Use in Pediatric Dentistry: A Review of Literature and A Recent UpdateTiaraNo ratings yet
- Comparative Assessment Between Eyelet Wiring and Direct Interdental Wiring For Achieving Intermaxillary Fixation A Prospective Randomized Clinical StuDocument5 pagesComparative Assessment Between Eyelet Wiring and Direct Interdental Wiring For Achieving Intermaxillary Fixation A Prospective Randomized Clinical StuAbhishek JhaNo ratings yet
- IntJPedodRehabil2260-4247839 114758Document6 pagesIntJPedodRehabil2260-4247839 114758anna handayaniNo ratings yet
- Calcium Hydroxide Induced Healing of Periapical RaDocument4 pagesCalcium Hydroxide Induced Healing of Periapical RaMaría José VanegasNo ratings yet
- Paroliaetal JIDDocument12 pagesParoliaetal JIDHaris KrnicNo ratings yet
- palatogingivalgrooveJIOH PDFDocument6 pagespalatogingivalgrooveJIOH PDFAthulya PallipurathNo ratings yet
- VYplastyDocument6 pagesVYplastyVineet ArunNo ratings yet
- Endodontic RadiologyFrom EverandEndodontic RadiologyBettina BasraniNo ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- Peerj 5258Document17 pagesPeerj 5258mmputraNo ratings yet
- CTG & FGG ComplicationDocument12 pagesCTG & FGG ComplicationmmputraNo ratings yet
- Oral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalDocument17 pagesOral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalmmputraNo ratings yet
- Microorganisms 09 02349Document12 pagesMicroorganisms 09 02349mmputraNo ratings yet
- Fcimb 09 00053Document11 pagesFcimb 09 00053mmputraNo ratings yet
- Review Article: Mixed Red-Complex Bacterial Infection in PeriodontitisDocument6 pagesReview Article: Mixed Red-Complex Bacterial Infection in PeriodontitismmputraNo ratings yet
- ContempClinDent 2013 4 4 437 123021Document8 pagesContempClinDent 2013 4 4 437 123021mmputraNo ratings yet
- Microbial Signatures of Health, Gingivitis, and PeriodontitisDocument22 pagesMicrobial Signatures of Health, Gingivitis, and PeriodontitismmputraNo ratings yet
- The Use of A Mobile App To Motivate Evidence-Based Oral Hygiene BehaviourDocument7 pagesThe Use of A Mobile App To Motivate Evidence-Based Oral Hygiene BehaviourmmputraNo ratings yet
- Micro Ora and Periodontal Disease: Dental Research Journal December 2012Document6 pagesMicro Ora and Periodontal Disease: Dental Research Journal December 2012mmputraNo ratings yet
- Jpis 48 22 1Document12 pagesJpis 48 22 1Aulia CahyaniNo ratings yet
- 10 6001@actamedica V24i3 3551-2Document9 pages10 6001@actamedica V24i3 3551-2mmputraNo ratings yet
- Guide to Managing Tooth Wear from AttritionDocument5 pagesGuide to Managing Tooth Wear from AttritionmmputraNo ratings yet
- Anatomi TMJDocument14 pagesAnatomi TMJmmputraNo ratings yet
- Creutzfeldt JakobDocument6 pagesCreutzfeldt JakobErnesto Ochoa MonroyNo ratings yet
- Why I Am Not A Primitivist - Jason McQuinnDocument9 pagesWhy I Am Not A Primitivist - Jason McQuinnfabio.coltroNo ratings yet
- Medical Instrumentation Application and Design 4th Edition Webster Solutions ManualDocument13 pagesMedical Instrumentation Application and Design 4th Edition Webster Solutions ManualSaraRogersrbwgd100% (15)
- Faith Surah RefutationDocument9 pagesFaith Surah RefutationKhairul Anuar Mohd IsaNo ratings yet
- Coding and Decoding Practice TestDocument13 pagesCoding and Decoding Practice TestRaja SubramanianNo ratings yet
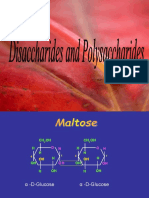
- Disaccharides and PolysaccharidesDocument17 pagesDisaccharides and PolysaccharidesAarthi shreeNo ratings yet
- Let's think step by step:- The common factor of 32, 45 and 50 is 5- 32/5 = 6.4 meters - 45/5 = 9 meters- 50/5 = 10 meters- So the best option is the 50 meter wire.b. How did you get the answerDocument59 pagesLet's think step by step:- The common factor of 32, 45 and 50 is 5- 32/5 = 6.4 meters - 45/5 = 9 meters- 50/5 = 10 meters- So the best option is the 50 meter wire.b. How did you get the answerjsphmnsycjrscribdNo ratings yet
- Aci 306.1Document5 pagesAci 306.1safak kahramanNo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- KF2.5-200 - With-M-C - GB - 03-15 KRACHT Bomba PDFDocument8 pagesKF2.5-200 - With-M-C - GB - 03-15 KRACHT Bomba PDFJairo Andrés FA100% (1)
- Early Daoist Dietary Practices: Examining Ways To Health and Longevity. by Shawn ArthurDocument6 pagesEarly Daoist Dietary Practices: Examining Ways To Health and Longevity. by Shawn ArthurlsdkNo ratings yet
- Candy Microwave OvenDocument31 pagesCandy Microwave OvencdimisNo ratings yet
- 74HCT00Document8 pages74HCT00Sadikul FuadNo ratings yet
- Developmental Screening Using The: Philippine Early Childhood Development ChecklistDocument30 pagesDevelopmental Screening Using The: Philippine Early Childhood Development ChecklistGene BonBonNo ratings yet
- Key Responsibilities On Skill.: Curriculum Vitae PersonalDocument3 pagesKey Responsibilities On Skill.: Curriculum Vitae PersonalLAM NYAWALNo ratings yet
- FisheryDocument2 pagesFisheryKyle GalangueNo ratings yet
- Al-Qawlul Mufeed: Backbiting and Its Impact On SocietyDocument2 pagesAl-Qawlul Mufeed: Backbiting and Its Impact On SocietyMountainofknowledgeNo ratings yet
- Soften, Soothe, AllowDocument1 pageSoften, Soothe, AllowTatiannaMartinsNo ratings yet
- Management The Essentials Australia 4th Edition Robbins Test BankDocument29 pagesManagement The Essentials Australia 4th Edition Robbins Test Bankfidelmanhangmhr100% (38)
- Class Record (Science 9) S.Y. 2020-2021Document8 pagesClass Record (Science 9) S.Y. 2020-2021Wilmar EspinosaNo ratings yet
- 1.0sg Equations and Inequalities - Study GuideDocument1 page1.0sg Equations and Inequalities - Study Guiderad58No ratings yet
- Bekkersdal Business Hive Close Out ReportDocument19 pagesBekkersdal Business Hive Close Out ReportMichael Benhura100% (2)
- R. Paul Wil - Rico ChetDocument7 pagesR. Paul Wil - Rico ChetJason Griffin100% (1)
- Detroit Cathedral Program Final 4-17-12Document2 pagesDetroit Cathedral Program Final 4-17-12Darryl BradleyNo ratings yet
- Albemarle Family YMCA Pool ScheduleDocument2 pagesAlbemarle Family YMCA Pool ScheduleYMCA of South Hampton RoadsNo ratings yet
- How To Make Nano Silica From Extracted Silica Rice Husk (Discussion)Document1 pageHow To Make Nano Silica From Extracted Silica Rice Husk (Discussion)MohdhafizFaiz MdAliNo ratings yet
- Moana Taka PartnershipDocument2 pagesMoana Taka Partnershipself sayidNo ratings yet
- 2009 - Mazars Insight Ifrs 5 enDocument36 pages2009 - Mazars Insight Ifrs 5 enSahar FekihNo ratings yet
- Cambodia's Rich Literary HeritageDocument5 pagesCambodia's Rich Literary HeritageChelle LancetaNo ratings yet
- Units 3 - 4 Workshop A2Document3 pagesUnits 3 - 4 Workshop A2S4N7Y PRONo ratings yet