You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1 Aerodynamics Lecture - Viscous FlowDocument70 pages1 Aerodynamics Lecture - Viscous Flowccoyure100% (2)
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- State of Stealth FINAL 121317Document41 pagesState of Stealth FINAL 121317Muhammad Afzaal100% (2)
- PAMDocument14 pagesPAMRashed IslamNo ratings yet
- Sarmatian Swords 2 - ROMECDocument12 pagesSarmatian Swords 2 - ROMECkulcsarv100% (2)
- Basic Labour Rate ListDocument6 pagesBasic Labour Rate ListmaheshNo ratings yet
- Artigo Introdução 02Document5 pagesArtigo Introdução 02ANA CAROLINE ANDRADE DE MELONo ratings yet
- Artigo Introdução 06Document32 pagesArtigo Introdução 06ANA CAROLINE ANDRADE DE MELONo ratings yet
- Artigo Introdução 05Document6 pagesArtigo Introdução 05ANA CAROLINE ANDRADE DE MELONo ratings yet
- 10.male Reproductive System 2 BlocksDocument220 pages10.male Reproductive System 2 BlocksANA CAROLINE ANDRADE DE MELONo ratings yet
- ShimadzuDocument66 pagesShimadzueka_setyowati0No ratings yet
- How To Write A Research Paper With Parenthetical DocumentationDocument5 pagesHow To Write A Research Paper With Parenthetical Documentationc9spy2qzNo ratings yet
- PT Activity 3.4.2: Troubleshooting A VLAN Implementation: Topology DiagramDocument3 pagesPT Activity 3.4.2: Troubleshooting A VLAN Implementation: Topology DiagramMatthew N Michelle BondocNo ratings yet
- Police Log July 30, 2016Document16 pagesPolice Log July 30, 2016MansfieldMAPoliceNo ratings yet
- Jurnal Milk Fever 3Document9 pagesJurnal Milk Fever 3darisNo ratings yet
- BB 3002Document2 pagesBB 3002Leslie TaylorNo ratings yet
- AE240 Notes Early-Airfoil-Development-Handout-1Document5 pagesAE240 Notes Early-Airfoil-Development-Handout-1mohamedNo ratings yet
- Theoretical Foundations of Nursing - Review MaterialDocument10 pagesTheoretical Foundations of Nursing - Review MaterialKennethNo ratings yet
- Radiation Physics and Chemistry: L.T. Hudson, J.F. SeelyDocument7 pagesRadiation Physics and Chemistry: L.T. Hudson, J.F. SeelyThư Phạm Nguyễn AnhNo ratings yet
- Numerology 666 Meaning: What Angel Number 666 REALLY Means!Document2 pagesNumerology 666 Meaning: What Angel Number 666 REALLY Means!LlNo ratings yet
- ActuatorsDocument24 pagesActuatorsharishcsharmaNo ratings yet
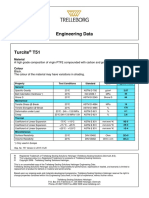
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Industrial Training Sample Report of Last YearDocument42 pagesIndustrial Training Sample Report of Last YearKetan NikamNo ratings yet
- 7th Chemistry DLP Study Package FinalDocument101 pages7th Chemistry DLP Study Package FinalAdityaNo ratings yet
- FMB70 Deltapilot S Medidor de Nivel HDocument44 pagesFMB70 Deltapilot S Medidor de Nivel HLICONSA MICHOACANNo ratings yet
- Manual HB ISM112 EDocument106 pagesManual HB ISM112 EALFAKNo ratings yet
- Design and Fabrication of Single Cylinder Solenoid EngineDocument7 pagesDesign and Fabrication of Single Cylinder Solenoid EngineVIVA-TECH IJRINo ratings yet
- Tecnical Data TYPE 139 L12R / L16RDocument1 pageTecnical Data TYPE 139 L12R / L16RLada LabusNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- Apacer SV250 CFast BiCS5 AA2 XX5XXX XXXEX Spec v1 - 3107344Document25 pagesApacer SV250 CFast BiCS5 AA2 XX5XXX XXXEX Spec v1 - 3107344ManunoghiNo ratings yet
- Smart Energy Meter and Monitoring System Using Iot IJERTCONV8IS14011Document4 pagesSmart Energy Meter and Monitoring System Using Iot IJERTCONV8IS14011Gurpreet SinghNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- Thank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842Document1 pageThank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842RuodNo ratings yet
- ETP Combined Spec - R0Document60 pagesETP Combined Spec - R0Pravash Chandra Senapaty100% (1)