You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- PCW Applicant's Information SheetDocument2 pagesPCW Applicant's Information SheetCielo Belen SandroNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AIT - PPO List As at September 2022 2Document9 pagesAIT - PPO List As at September 2022 2Guilherme Ventura100% (1)
- Case Scenario 1: Making Decision Based Upon The Situation (Paternalism and Utilitarianism)Document2 pagesCase Scenario 1: Making Decision Based Upon The Situation (Paternalism and Utilitarianism)Heart BeatingNo ratings yet
- Sushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Document1 pageSushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Ganesh ganiNo ratings yet
- Is Oet Accepted in Usa - Google SearchDocument1 pageIs Oet Accepted in Usa - Google SearchJune Mark Reyes AlferezNo ratings yet
- Informatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseDocument5 pagesInformatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseKevin SangNo ratings yet
- Curriculum Vitae For Mrs Alita Gloria MpingaDocument9 pagesCurriculum Vitae For Mrs Alita Gloria Mpingaalita ngomaneNo ratings yet
- Payslip For March 2023 - TORM ARAWA (Closed Payroll) : Torm A/S Torm A/SDocument1 pagePayslip For March 2023 - TORM ARAWA (Closed Payroll) : Torm A/S Torm A/SRodelio TomasNo ratings yet
- DHA ExamDocument7 pagesDHA ExamMaraj Raees khan Mohd MarajNo ratings yet
- Cost Effectiveness in Medical EducationDocument43 pagesCost Effectiveness in Medical EducationMarco OliveiraNo ratings yet
- University of The Philippines Manila College of MedicineDocument3 pagesUniversity of The Philippines Manila College of MedicineDhian MorishitaNo ratings yet
- List of Approved Schools With Admission QuotaDocument21 pagesList of Approved Schools With Admission QuotaAdegboye AdedayoNo ratings yet
- Bill Cum Receipt - Ms Humki Devi .Document1 pageBill Cum Receipt - Ms Humki Devi .Rahul SsdotraNo ratings yet
- Phc-Ii Final Exams-2021Document5 pagesPhc-Ii Final Exams-2021Galakpai KolubahNo ratings yet
- The 'S of CSW BillingDocument2 pagesThe 'S of CSW Billingmamatha mamtaNo ratings yet
- UntitledDocument133 pagesUntitledMalou Bautista-EscanerNo ratings yet
- Date Performed Patient's Name Procedure Performed OR Nurse On Duty Supervised byDocument2 pagesDate Performed Patient's Name Procedure Performed OR Nurse On Duty Supervised byjames pasionNo ratings yet
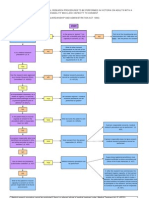
- Approval Process For Medical Research FlowchartDocument1 pageApproval Process For Medical Research FlowchartabcdcattigerNo ratings yet
- Chn-Health-Related Activities in The CommunityDocument3 pagesChn-Health-Related Activities in The CommunityBSN 1-N CASTRO, RicciNo ratings yet
- MedicaidDocument2 pagesMedicaidgeorge josephNo ratings yet
- The Role of Primary Health Care in NigeriaDocument6 pagesThe Role of Primary Health Care in NigeriaGreat OdineNo ratings yet
- OPD Action PlanDocument6 pagesOPD Action PlanTAHIR NURINo ratings yet
- Delegate List: Amanda-Jane ErneDocument20 pagesDelegate List: Amanda-Jane ErneDebjani DuttaNo ratings yet
- Minimum Wage Board 2013 Publishes GazetteDocument3 pagesMinimum Wage Board 2013 Publishes GazetteMahiulhabibNo ratings yet
- NHS FPX 6008 Assessment 2 Needs Analysis For ChangeDocument7 pagesNHS FPX 6008 Assessment 2 Needs Analysis For Changefarwaamjad771No ratings yet
- Saudi Family NetworkDocument232 pagesSaudi Family NetworkIbrahim Ansari 2218073No ratings yet
- Questionnaire - 7853582Document1 pageQuestionnaire - 7853582SMLD Nursing SchoolNo ratings yet
- IELTS Listening Practice Test 5: Section 1Document9 pagesIELTS Listening Practice Test 5: Section 1HoaiNhiNguyenNo ratings yet
- Pharmacy Exam OdishaDocument1 pagePharmacy Exam Odishasimpurock001No ratings yet
- Role Play Helping With Rehabilitation - Group 4 - 2aDocument12 pagesRole Play Helping With Rehabilitation - Group 4 - 2aAbang GotenNo ratings yet