You might also like
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (6)
- Congestive Cardiac Failure GuideDocument47 pagesCongestive Cardiac Failure GuideRajesh Sharma100% (1)
- AAN 204 CARDIOVASCULAR NURSING COURSEWORKDocument118 pagesAAN 204 CARDIOVASCULAR NURSING COURSEWORKLucian CaelumNo ratings yet
- Atrial Fibrillation (AF)Document24 pagesAtrial Fibrillation (AF)farmasi_hm100% (1)
- 3.preoperative Patient Assessment and ManagementDocument76 pages3.preoperative Patient Assessment and Managementoliyad alemayehuNo ratings yet
- Diagnosis and Management of HypertensionDocument35 pagesDiagnosis and Management of HypertensionBasil Hussam100% (2)
- Essentials of Community Medicine - A Practical Approach PDFDocument487 pagesEssentials of Community Medicine - A Practical Approach PDFamarhadid70% (20)
- Management of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthDocument71 pagesManagement of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthPrincewill SeiyefaNo ratings yet
- Helene Deutsch, A Psychoanalysts Life (Lacanempdf)Document400 pagesHelene Deutsch, A Psychoanalysts Life (Lacanempdf)Carlos AugustoNo ratings yet
- Being in The World Selected Pa Ludwig BinswangerDocument388 pagesBeing in The World Selected Pa Ludwig BinswangerRamazan ÇarkıNo ratings yet
- National Clinical Pharmacy Service Implementation ManualDocument112 pagesNational Clinical Pharmacy Service Implementation ManualAbdulhakim ZekeriyaNo ratings yet
- Atrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhDocument45 pagesAtrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- Introduction: A New Hierarchy of NeedsDocument5 pagesIntroduction: A New Hierarchy of Needsgun2 block100% (1)
- Heart FailureDocument28 pagesHeart FailureaparnaNo ratings yet
- CH 33 Key PointsDocument4 pagesCH 33 Key PointsKara Dawn MasonNo ratings yet
- Hypertension ESC Guideline 2018Document78 pagesHypertension ESC Guideline 2018Theresia KennyNo ratings yet
- Hypertension Guideline SummaryDocument12 pagesHypertension Guideline Summaryمصطفى ابراهيم سعيدNo ratings yet
- Diabetes and Peripheral Artery DiseaseDocument30 pagesDiabetes and Peripheral Artery DiseasedrbrdasNo ratings yet
- Cardiovascular Disease in The ElderlyDocument18 pagesCardiovascular Disease in The ElderlynfacmaNo ratings yet
- Hypertension: Silent KillerDocument28 pagesHypertension: Silent KilleribratiNo ratings yet
- Hypertension 2019 PDFDocument46 pagesHypertension 2019 PDFPNo ratings yet
- Medically Compromised Patient: HypertensionDocument32 pagesMedically Compromised Patient: Hypertensionمحمد عبدالهادي إسماعيلNo ratings yet
- Antihypertensive Drugs GuideDocument52 pagesAntihypertensive Drugs GuideAlan LealNo ratings yet
- Pharmacotherapy - Hypertension - Dr. Mohammed KamalDocument85 pagesPharmacotherapy - Hypertension - Dr. Mohammed KamalMohammed KamalNo ratings yet
- Hypertension: Dr. Lucia Mazur-Nicorici Md. PHDDocument34 pagesHypertension: Dr. Lucia Mazur-Nicorici Md. PHDValerianBîcosNo ratings yet
- Hypertension GuideDocument25 pagesHypertension GuideBulborea MihaelaNo ratings yet
- HypertensionDocument45 pagesHypertensionM Farhad KhaniNo ratings yet
- HypertensionDocument10 pagesHypertensionaa zzNo ratings yet
- Hypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Document81 pagesHypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Alan K MhamadNo ratings yet
- Cardiovascular Agents PDFDocument118 pagesCardiovascular Agents PDFgherlethrNo ratings yet
- Diabetes HypertensionDocument29 pagesDiabetes HypertensionAnimesh PaulNo ratings yet
- HypertensionDocument58 pagesHypertensionSHAHALOMGIR AHMEDNo ratings yet
- Stroke Prevention and Management Guideline SummaryDocument24 pagesStroke Prevention and Management Guideline Summarynisha24100% (1)
- Hypertension: Prepared By: Dr. Shadab Kashif R.PH, M.SC (UK)Document18 pagesHypertension: Prepared By: Dr. Shadab Kashif R.PH, M.SC (UK)Ahmad Jamal HashmiNo ratings yet
- DocumentDocument10 pagesDocumentMulhma AlharbiNo ratings yet
- Management of HypertensionDocument67 pagesManagement of Hypertensionainzahir94No ratings yet
- 3 HypertensionDocument26 pages3 Hypertensionsamar yousif mohamedNo ratings yet
- Jurnal Reading 2Document14 pagesJurnal Reading 2Riko KuswaraNo ratings yet
- Increased Arterial Blood PressureDocument25 pagesIncreased Arterial Blood PressureAjmalNo ratings yet
- Pharmacotherapy of HypertensionDocument52 pagesPharmacotherapy of HypertensionDrVinod Kumar Goud VemulaNo ratings yet
- Pathophysiology: Cardiovascular System Dr. Maen DweikDocument38 pagesPathophysiology: Cardiovascular System Dr. Maen DweikshoibyNo ratings yet
- Heartfailurepptsam 170511135108Document48 pagesHeartfailurepptsam 170511135108enam professorNo ratings yet
- Myocardial InfarctionDocument5 pagesMyocardial InfarctionNikki MacasaetNo ratings yet
- Ch. 32 - Hypertension - EditedDocument43 pagesCh. 32 - Hypertension - Editedمحمد الحواجرةNo ratings yet
- Hypertension HTNDocument42 pagesHypertension HTNpeter dymonNo ratings yet
- HypertensionDocument14 pagesHypertensiondrraziawardakNo ratings yet
- B HypertensionDocument15 pagesB Hypertensionabotawfeq abojalilNo ratings yet
- تقرير ضغط الدمDocument10 pagesتقرير ضغط الدمlyh355754No ratings yet
- Resumen The Seventh Report of The JointDocument4 pagesResumen The Seventh Report of The JointMARIANA GARCIA LOPEZNo ratings yet
- Clinical Research: Hypertension ManagementDocument4 pagesClinical Research: Hypertension ManagementJay Linus Rante SanchezNo ratings yet
- Farmakoterapi StrokeDocument33 pagesFarmakoterapi StrokeMuhammad Aldi SetiawanNo ratings yet
- Sudden Cardiac Arrest: DiscussionDocument19 pagesSudden Cardiac Arrest: DiscussionIza Singson-CristobalNo ratings yet
- CVS DOs RevisedDocument88 pagesCVS DOs RevisedTaate MohammedNo ratings yet
- Hypertensive CrisisDocument60 pagesHypertensive CrisisDzikrul Haq KarimullahNo ratings yet
- Osamah Ischemic StrokeDocument37 pagesOsamah Ischemic Strokejana.alngNo ratings yet
- Oral Health Considerations in Hypertensive Patient: Abhishikth Abraham Varghese Final Year Part 1 180020531Document21 pagesOral Health Considerations in Hypertensive Patient: Abhishikth Abraham Varghese Final Year Part 1 180020531Abhishikth VargheseNo ratings yet
- Atrial FibrillationDocument50 pagesAtrial Fibrillationkapil khanalNo ratings yet
- End-Stage Heart Disease Management and Palliative Care GuidelinesDocument44 pagesEnd-Stage Heart Disease Management and Palliative Care GuidelinesCyrille AgnesNo ratings yet
- Arrhythimas 6Document38 pagesArrhythimas 6غفران هيثم خليلNo ratings yet
- Kee: Pharmacology, 8th EditionDocument5 pagesKee: Pharmacology, 8th EditionLondera BainNo ratings yet
- Hypertension Lecture3: Pharmacological TreatmentDocument25 pagesHypertension Lecture3: Pharmacological TreatmentRam NiwasNo ratings yet
- Neurologic Function Cerebrovascular DisordersDocument15 pagesNeurologic Function Cerebrovascular DisordersBalilea, Derwin Stephen T.No ratings yet
- The Overview of Hypertension 2009Document50 pagesThe Overview of Hypertension 2009YeniNo ratings yet
- Anti-Hypertensive 2Document49 pagesAnti-Hypertensive 2pushpaNo ratings yet
- Medical Nutrition Therapy For Cardiovascular Disease 2013Document30 pagesMedical Nutrition Therapy For Cardiovascular Disease 2013ashry909100% (1)
- Unveiling the Unseen: A Journey Into the Hearts Labyrinth SeanFrom EverandUnveiling the Unseen: A Journey Into the Hearts Labyrinth SeanNo ratings yet
- Physical Assi1Document26 pagesPhysical Assi1Abdulhakim ZekeriyaNo ratings yet
- Cology PageDocument4 pagesCology PageAbdulhakim ZekeriyaNo ratings yet
- History of Drug Discovery 1Document7 pagesHistory of Drug Discovery 1Brent FontanillaNo ratings yet
- Histology: Diagnosis and Treatment of Chronic Apical AbscessDocument3 pagesHistology: Diagnosis and Treatment of Chronic Apical AbscessPrince AmiryNo ratings yet
- 6.11 Bullying ReadyDocument41 pages6.11 Bullying ReadyAstraX EducationNo ratings yet
- BA Euroflyer Direct Entry Pilot - Captain A320 at British AirwaysDocument1 pageBA Euroflyer Direct Entry Pilot - Captain A320 at British AirwaysdifjdjdjNo ratings yet
- Nur3116 Social Determinants of Health PaperDocument6 pagesNur3116 Social Determinants of Health Paperapi-578141969No ratings yet
- Title: Re-Gala: Rationale:: Emiliano Gala Elementary SchoolDocument2 pagesTitle: Re-Gala: Rationale:: Emiliano Gala Elementary SchoolReign Magadia BautistaNo ratings yet
- Beliefs About Obsessional Thoughts InventoryDocument21 pagesBeliefs About Obsessional Thoughts InventoryMarta CerdáNo ratings yet
- Identifying topic and supporting sentencesDocument3 pagesIdentifying topic and supporting sentencesRizkiNo ratings yet
- ReportingDocument4 pagesReportingMark CalimlimNo ratings yet
- Material Safety Data Sheet Material Safety Data SheetDocument3 pagesMaterial Safety Data Sheet Material Safety Data SheetKarthik0% (2)
- Subject: Submission of Deficient Information / Documents: F.No.10-10/2020-OTC) (M-82)Document107 pagesSubject: Submission of Deficient Information / Documents: F.No.10-10/2020-OTC) (M-82)Saad PathanNo ratings yet
- Sex Education Literacy Stem 11 A.Document54 pagesSex Education Literacy Stem 11 A.Bangtan SeonyeondanNo ratings yet
- Confounding Variables: Ali Yassin and Bara'a Jardali Presented To Dr. Issam I. ShaaraniDocument12 pagesConfounding Variables: Ali Yassin and Bara'a Jardali Presented To Dr. Issam I. ShaaraniAli GhanemNo ratings yet
- Hts Policy PhilippinesDocument15 pagesHts Policy PhilippinesBrunxAlabastro100% (1)
- Writing Sample 2Document9 pagesWriting Sample 2api-582848179No ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
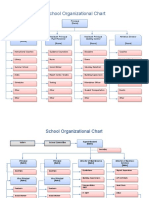
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- CIL Recruitment for 66 Medical Executive PostsDocument12 pagesCIL Recruitment for 66 Medical Executive PostsTaseemNo ratings yet
- Improving Project ProposalsDocument2 pagesImproving Project ProposalsNancy Nicasio SanchezNo ratings yet
- Digital Citizenship vs. Global CitizenshipDocument20 pagesDigital Citizenship vs. Global CitizenshipMacasinag Jamie Anne M.No ratings yet
- Sodium Bicarbonate: PresentationDocument3 pagesSodium Bicarbonate: Presentationmadimadi11No ratings yet
- 27 Annual ReportDocument102 pages27 Annual Reportudiptya_papai2007No ratings yet
- PRA Tool Box: 6.1. Brief Introduction To PRADocument16 pagesPRA Tool Box: 6.1. Brief Introduction To PRAfaisalNo ratings yet
- Validate Questionnaire on Physical ActivitiesDocument2 pagesValidate Questionnaire on Physical ActivitiesSamantha AceraNo ratings yet
- DD - DA Li Ion MSDS U80277 2R2 - SDS 2018Document5 pagesDD - DA Li Ion MSDS U80277 2R2 - SDS 2018lintangscribdNo ratings yet
- A Concept-Based Approach To Learning: DevelopmentDocument62 pagesA Concept-Based Approach To Learning: DevelopmentAli Nawaz AyubiNo ratings yet