You might also like
- Pedia 1Document8 pagesPedia 1Jani MisterioNo ratings yet
- Case Presentation DraftDocument6 pagesCase Presentation DraftGwendareign ElizanNo ratings yet
- SGD October 15 JIDocument5 pagesSGD October 15 JIRay Emmanuel Enriquez DomingoNo ratings yet
- Long Case - Labiqatullubabah-En LokalDocument14 pagesLong Case - Labiqatullubabah-En LokalHendra WardhanaNo ratings yet
- EN - Vita Pramatasari (Rev Miss Aini)Document20 pagesEN - Vita Pramatasari (Rev Miss Aini)Hendra WardhanaNo ratings yet
- Obstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Document6 pagesObstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Justin LamNo ratings yet
- Kasus Perdarahan Intrakranial Pada Bayi Baru LahirDocument58 pagesKasus Perdarahan Intrakranial Pada Bayi Baru LahirSilvia PAgitta TariganNo ratings yet
- 1 Month Old Baby with Intracranial HemorrhageDocument58 pages1 Month Old Baby with Intracranial HemorrhageRechax Squad RezapawelloiNo ratings yet
- Bedside DHF Grade 1Document42 pagesBedside DHF Grade 1reshianeNo ratings yet
- ROSIMO - AUG 2021 NB VomitingDocument5 pagesROSIMO - AUG 2021 NB VomitingcarlosNo ratings yet
- Daily Platelet Monitoring in DengueDocument52 pagesDaily Platelet Monitoring in DengueIrfan Dzakir NugrohoNo ratings yet
- CC 13 October 2017 (Demam Neutropenia) 2Document35 pagesCC 13 October 2017 (Demam Neutropenia) 2febrydwiNo ratings yet
- Case Management NICU July 2020 Sam WibowoDocument6 pagesCase Management NICU July 2020 Sam WibowoSamuel WibowoNo ratings yet
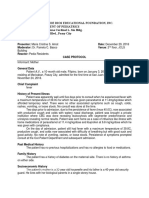
- San Juan de Dios Educational Foundation, Inc. Department of Pediatrics 4th Floor Jaime Cardinal L. Sin Bldg. 2772 Roxas BLVD., Pasay CityDocument5 pagesSan Juan de Dios Educational Foundation, Inc. Department of Pediatrics 4th Floor Jaime Cardinal L. Sin Bldg. 2772 Roxas BLVD., Pasay CityNiña AmatNo ratings yet
- Hirschsprung'S Disease in A Child: Case ReportDocument57 pagesHirschsprung'S Disease in A Child: Case ReportHans NatanaelNo ratings yet
- Case Report Vacuum Extraction Due To Prolonged Second Stage of LaborDocument20 pagesCase Report Vacuum Extraction Due To Prolonged Second Stage of Laborverga0% (1)
- CC 4 Nov 2017 SeizureDocument44 pagesCC 4 Nov 2017 SeizurenisaNo ratings yet
- Integration Activity 3 PDFDocument18 pagesIntegration Activity 3 PDFCzarinaNo ratings yet
- Pneumonia PedsDocument13 pagesPneumonia PedsRSNo ratings yet
- National Board Examination - Kiki Dwi QoriDocument18 pagesNational Board Examination - Kiki Dwi QoriHendra WardhanaNo ratings yet
- ABNORMAL ASSESSMENT OF NEWBORNDocument7 pagesABNORMAL ASSESSMENT OF NEWBORNPriyaNo ratings yet
- Case Study 1Document13 pagesCase Study 1Kiana TehraniNo ratings yet
- Preskas BedahDocument15 pagesPreskas BedahnabilahfajriahNo ratings yet
- Congenital Pneumonia Case ReportDocument17 pagesCongenital Pneumonia Case ReportHendra WardhanaNo ratings yet
- Morning Report CF + UTIDocument35 pagesMorning Report CF + UTIdr.ronak1996No ratings yet
- Morning Report CFDocument33 pagesMorning Report CFdr.ronak1996No ratings yet
- CC 10 NOv 2017 ITPDocument32 pagesCC 10 NOv 2017 ITPLilik NatasubrataNo ratings yet
- Long Case - Susilowati (En Lokal)Document17 pagesLong Case - Susilowati (En Lokal)Hendra WardhanaNo ratings yet
- Case Conference on Anemia PatientDocument35 pagesCase Conference on Anemia PatientAisya FikritamaNo ratings yet
- Hashim Major LogDocument26 pagesHashim Major LogHashim AlsammawiNo ratings yet
- Pediatric Case History of Acute Respiratory IllnessDocument8 pagesPediatric Case History of Acute Respiratory IllnessFatemeh BemanaNo ratings yet
- Presentation Palatal MassDocument41 pagesPresentation Palatal MassAmit AnandNo ratings yet
- 6 POSTNATAL Case - Book Rupi - OBS p367-534Document168 pages6 POSTNATAL Case - Book Rupi - OBS p367-534piyush0751100% (1)
- CASE CONFERENCE FOR PEDIATRIC PATIENTSDocument39 pagesCASE CONFERENCE FOR PEDIATRIC PATIENTSAisya FikritamaNo ratings yet
- medical report - PneumoniaeDocument8 pagesmedical report - Pneumoniaenguyenhoavanchi2002No ratings yet
- PCC CaseDocument9 pagesPCC CaseKaila AbeledaNo ratings yet
- Easter College: Department of NursingDocument13 pagesEaster College: Department of NursingShaii shanNo ratings yet
- CC 4 Nov 2017 SeizureDocument44 pagesCC 4 Nov 2017 SeizureLilik NatasubrataNo ratings yet
- Shazia CM On 02.09.20 CorrectedDocument59 pagesShazia CM On 02.09.20 CorrectedShazia Afreen TonniNo ratings yet
- Syphilis in Pregnancy Case ReportDocument28 pagesSyphilis in Pregnancy Case ReportmuhammadrubaiNo ratings yet
- Nursing Care Plan for Neonate with Low Birth WeightDocument14 pagesNursing Care Plan for Neonate with Low Birth WeightArchna Yadav100% (1)
- ASUHAN KEPERAWATAN HIPERBILIRUBINDocument13 pagesASUHAN KEPERAWATAN HIPERBILIRUBINRenanda Dika MNo ratings yet
- Clerk GCPDocument19 pagesClerk GCPNikki DiocampoNo ratings yet
- Case Report on a 23-Month-Old Boy with Grade I Dengue Hemorrhagic FeverDocument49 pagesCase Report on a 23-Month-Old Boy with Grade I Dengue Hemorrhagic FeverPashëm IndonesiaNo ratings yet
- Baby E.N. Case ReportDocument4 pagesBaby E.N. Case ReportKemotherapy LifesucksNo ratings yet
- ABO Incompatibility in NeonateDocument27 pagesABO Incompatibility in NeonatemarshalitaNo ratings yet
- CC 5 October 2017 W JDocument39 pagesCC 5 October 2017 W JLilik NatasubrataNo ratings yet
- Case Conference Friday Shift, June 30 2017Document49 pagesCase Conference Friday Shift, June 30 2017Izni AyuniNo ratings yet
- Grand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianDocument65 pagesGrand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianJessa MeaNo ratings yet
- Buat CaseDocument13 pagesBuat CaseBima Sena Arya YudhaNo ratings yet
- "Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaDocument20 pages"Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaNikki DiocampoNo ratings yet
- Liver Abscess Risk FactorsDocument7 pagesLiver Abscess Risk FactorsJoan junioNo ratings yet
- Lapjag 10 Maret 19Document2 pagesLapjag 10 Maret 19Bernardo Daniel LawrenciusNo ratings yet
- Exam Ticket Number Wise CaseDocument37 pagesExam Ticket Number Wise CaseVikrantNo ratings yet
- Intestinal Obstruction E.C Atresia IleumDocument12 pagesIntestinal Obstruction E.C Atresia IleumRobert ChristevenNo ratings yet
- CC 17 Feb 2017 1st Epilepsy OkeDocument43 pagesCC 17 Feb 2017 1st Epilepsy OkeLucky Yoga -satria NatasukmaNo ratings yet
- Case Management Protocol-Ong-Centipede Envenomation FINALDocument5 pagesCase Management Protocol-Ong-Centipede Envenomation FINALSamuel WibowoNo ratings yet
- Case Protocol OB - H MOLEDocument3 pagesCase Protocol OB - H MOLEKim Adarem Joy ManimtimNo ratings yet
- MR 31 Jan 2021 - BronkopneumoniaDocument30 pagesMR 31 Jan 2021 - Bronkopneumoniagalihrahman51No ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Statement of The ProblemDocument1 pageStatement of The ProblemGwendareign ElizanNo ratings yet
- Patient History Source of Information (Reliability) : GRANDMOTHER and Neighbor (70%) Source of Referral: None General DataDocument8 pagesPatient History Source of Information (Reliability) : GRANDMOTHER and Neighbor (70%) Source of Referral: None General DataGwendareign ElizanNo ratings yet
- UP Manila Disorders of Adrenal CortexDocument3 pagesUP Manila Disorders of Adrenal CortexGwendareign ElizanNo ratings yet
- 1Document6 pages1Gwendareign ElizanNo ratings yet
- Documentary Requirements For HRH 2019: Director IV Provincial DOH OfficerDocument1 pageDocumentary Requirements For HRH 2019: Director IV Provincial DOH OfficerGwendareign ElizanNo ratings yet
- Sample PdsDocument4 pagesSample PdsGwendareign ElizanNo ratings yet
- Deployment Program Application Form Revision 0 (New) PDFDocument1 pageDeployment Program Application Form Revision 0 (New) PDFGwendareign ElizanNo ratings yet
- Personal Data SheetDocument16 pagesPersonal Data SheetGwendareign ElizanNo ratings yet
- Campus Nurse Application LetterDocument1 pageCampus Nurse Application LetterGwendareign ElizanNo ratings yet
- Deployment Program Application Form Revision 0 (New)Document1 pageDeployment Program Application Form Revision 0 (New)Gwendareign ElizanNo ratings yet
- NMAT supplementary handout provides medical school codesDocument2 pagesNMAT supplementary handout provides medical school codesjay5ar5jamorabon5torNo ratings yet
- SERVICE LEAVE PLANNING FOR BARANGAYS SOROC, SAN MATEO AND SAN ANDRES, BORONGAN CITY (JAN-APR 2017Document8 pagesSERVICE LEAVE PLANNING FOR BARANGAYS SOROC, SAN MATEO AND SAN ANDRES, BORONGAN CITY (JAN-APR 2017Gwendareign ElizanNo ratings yet
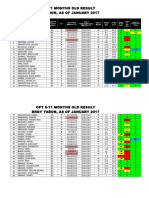
- Opt 0-71 Months Old Result Brgy Yabon, As of January 2017Document2 pagesOpt 0-71 Months Old Result Brgy Yabon, As of January 2017Gwendareign ElizanNo ratings yet
- Elderly Masterlist 60 Years Old and Above Brgy Yabon, Brgy Canano and Brgy BinobucalanDocument8 pagesElderly Masterlist 60 Years Old and Above Brgy Yabon, Brgy Canano and Brgy BinobucalanGwendareign ElizanNo ratings yet
- TB in PinasDocument2 pagesTB in PinasGwendareign ElizanNo ratings yet
- Guyabano Dry Sampling Justmar OkDocument2 pagesGuyabano Dry Sampling Justmar OkGwendareign ElizanNo ratings yet
- Target client list for family planningDocument3 pagesTarget client list for family planningGwendareign ElizanNo ratings yet
- BasketballDocument37 pagesBasketballGwendareign ElizanNo ratings yet
- Distance EducationDocument15 pagesDistance EducationGwendareign ElizanNo ratings yet
- NURSING CARE PLAN-case PresDocument24 pagesNURSING CARE PLAN-case PresGwendareign ElizanNo ratings yet
- Essential Newborn Care ProtocolDocument30 pagesEssential Newborn Care ProtocolGwendareign ElizanNo ratings yet
- Naig Pharma StudyDocument4 pagesNaig Pharma StudyGwendareign ElizanNo ratings yet
- Neonatal Infections BendelDocument89 pagesNeonatal Infections BendelRomica MarcanNo ratings yet
- Neonatal SepsisDocument17 pagesNeonatal SepsisDhilla Feroh Kesuma TNo ratings yet
- Lesson Plan On Neonatal InfectionDocument12 pagesLesson Plan On Neonatal InfectionMansiNo ratings yet
- Mid TermDocument17 pagesMid TermTamoghna NaskarNo ratings yet
- Case Study: Neonatal PneumoniaDocument47 pagesCase Study: Neonatal PneumoniaJay Villasoto100% (1)
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- Neonatal Infections Part 1 - MDM DygDocument30 pagesNeonatal Infections Part 1 - MDM DygNana YunusNo ratings yet
- (Journal of Perinatal Medicine) Management of Prelabour Rupture of Membranes (PROM) at TermDocument3 pages(Journal of Perinatal Medicine) Management of Prelabour Rupture of Membranes (PROM) at TermSofri m.tahirNo ratings yet
- MeningitisDocument244 pagesMeningitisputusanggraNo ratings yet
- Tog 12091Document4 pagesTog 12091princessmeleana6499No ratings yet
- Early Use of Antibiotics Is Associated With A Lower Incidence of Necrotizing EnterocolitisDocument9 pagesEarly Use of Antibiotics Is Associated With A Lower Incidence of Necrotizing EnterocolitisRestu TriwulandaniNo ratings yet
- Unit Plan Nursing ManagementDocument4 pagesUnit Plan Nursing ManagementSURAJ2792100% (1)
- Neonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollDocument9 pagesNeonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollMarco Antonio Mendoza OjedaNo ratings yet
- Advances in Neonatal InfectionsDocument5 pagesAdvances in Neonatal InfectionsElizabeth HendersonNo ratings yet
- Perinatal Infections GuideDocument24 pagesPerinatal Infections GuideAlexandra OanaNo ratings yet
- Newborn Sepsis: Causes, Risks and Prevention in InfantsDocument19 pagesNewborn Sepsis: Causes, Risks and Prevention in InfantsLekshmi ManuNo ratings yet
- Neonatology Clinical Treatment Guidelines OTHER VERSIONDocument94 pagesNeonatology Clinical Treatment Guidelines OTHER VERSIONAlexandraelsaNo ratings yet
- NCM 109 Lec MidtermsDocument8 pagesNCM 109 Lec MidtermsAngel Kim MalabananNo ratings yet
- ChorioamnionitisDocument22 pagesChorioamnionitisBrigita De VegaNo ratings yet
- Ajp - 180544 EosDocument9 pagesAjp - 180544 EosJeeNo ratings yet
- Review of Neonatal Sepsis Causes, Risk Factors and ManagementDocument9 pagesReview of Neonatal Sepsis Causes, Risk Factors and ManagementTiwi QiraNo ratings yet
- Neonatal InfectionsDocument18 pagesNeonatal InfectionsSanthosh.S.U100% (1)
- Neonatal SepsisDocument22 pagesNeonatal Sepsisjake1014100% (1)
- Antibiotics For Prelabour Rupture of Membranes at or Near Term (Review)Document71 pagesAntibiotics For Prelabour Rupture of Membranes at or Near Term (Review)Fatwa MNo ratings yet
- Garcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Document3 pagesGarcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Mushy_ayaNo ratings yet
- Sepsis Neonatorum PDFDocument2 pagesSepsis Neonatorum PDFAri Julian SaputraNo ratings yet
- Antibiotic-Guideline-for-Neonatal SepsisDocument13 pagesAntibiotic-Guideline-for-Neonatal SepsisNada AhmedNo ratings yet
- POGI Infection in Pregnancy 2022Document93 pagesPOGI Infection in Pregnancy 2022SDM RSTINo ratings yet
- Neonatal SepsisDocument39 pagesNeonatal SepsisBryan KernsNo ratings yet
- Neonatal InfectionDocument9 pagesNeonatal InfectionnishaNo ratings yet