You might also like
- Faisalabad Institute of Cardiology, Faisalabad.: Discharge SlipDocument1 pageFaisalabad Institute of Cardiology, Faisalabad.: Discharge SlipFarhanNo ratings yet
- This Study Resource Was: Cardiogenic ShockDocument5 pagesThis Study Resource Was: Cardiogenic ShockShyla Manguiat100% (1)
- ACLS Study GuideDocument305 pagesACLS Study GuideRahma Rafina100% (2)
- Electrophysiology StudyDocument84 pagesElectrophysiology StudySarni100% (2)
- Cardiac ArrhythmiasDocument4 pagesCardiac Arrhythmiassmurf096No ratings yet
- Prevalence of Dyslipidemia in Patients With Acute Coronary Syndrome Admitted at Tertiary Care Hospital in Nepal: A Descriptive Cross-Sectional StudyDocument10 pagesPrevalence of Dyslipidemia in Patients With Acute Coronary Syndrome Admitted at Tertiary Care Hospital in Nepal: A Descriptive Cross-Sectional StudybilahalvirayuNo ratings yet
- Poster 2020 DuphatDocument2 pagesPoster 2020 DuphatrajkumarrajendramNo ratings yet
- Effect of Oil Sacha InchiDocument5 pagesEffect of Oil Sacha InchiCinthia Huamaní GamunalNo ratings yet
- Sedentary Lifestyle and Antecedents of Cardiovascular Disease in Young AdultsDocument7 pagesSedentary Lifestyle and Antecedents of Cardiovascular Disease in Young AdultsmajidhalimwNo ratings yet
- Prevalence of Hypothyroidism in Patients With Chronic Kidney Disease: A Cross-Sectional Study From North IndiaDocument4 pagesPrevalence of Hypothyroidism in Patients With Chronic Kidney Disease: A Cross-Sectional Study From North IndiaReuben JosephNo ratings yet
- Once-Weekly Semaglutide in Adults With Overweight or ObesityDocument34 pagesOnce-Weekly Semaglutide in Adults With Overweight or ObesityRIJO CHERIANNo ratings yet
- Gliptins: Current Status & Future PromiseDocument46 pagesGliptins: Current Status & Future PromiseSmit ShahNo ratings yet
- Inadequate Glycaemic Control and Therapeutic Management of Adults Over 65 Years Old With Type 2 Diabetes Mellitus in SpainDocument6 pagesInadequate Glycaemic Control and Therapeutic Management of Adults Over 65 Years Old With Type 2 Diabetes Mellitus in SpainDaniel BenitezNo ratings yet
- Valeriaceci 15 Atefi 5854Document8 pagesValeriaceci 15 Atefi 5854Irish S. PonceNo ratings yet
- Metabolic Syndrome in Newly-Diagnosed Type 2 Dabetes: Md. Nguyeãn Thò Thu Thaûo Prof - Phd. Nguyeãn Thy KhueâDocument27 pagesMetabolic Syndrome in Newly-Diagnosed Type 2 Dabetes: Md. Nguyeãn Thò Thu Thaûo Prof - Phd. Nguyeãn Thy KhueâNhất ThanhNo ratings yet
- Slide Curriculum Diabetes and CardiologyDocument52 pagesSlide Curriculum Diabetes and CardiologyNazmul Hasan MahmudNo ratings yet
- The MERCURY I OpenDocument12 pagesThe MERCURY I OpenSharmil IyapillaiNo ratings yet
- 2016 Article 69Document10 pages2016 Article 69Rhowy Al-mu'izzahNo ratings yet
- GlucoseDocument5 pagesGlucosebagsouravNo ratings yet
- EUA 2019 Outcomes of SGLT2 Inhibitors Use in Diabetic RenalDocument4 pagesEUA 2019 Outcomes of SGLT2 Inhibitors Use in Diabetic RenalLaura GarciaNo ratings yet
- Kartoun Amia July 9 2015 FinalDocument2 pagesKartoun Amia July 9 2015 FinalUKNo ratings yet
- Diabetes Mellitus Etiology Pathogenesis Clinical FormsDocument73 pagesDiabetes Mellitus Etiology Pathogenesis Clinical FormsChanti Jessica RavaniNo ratings yet
- Lipid Profile in CKDDocument4 pagesLipid Profile in CKDAmiyanshu BeheraNo ratings yet
- A Comprehensive Review On Metabolic SyndromeDocument36 pagesA Comprehensive Review On Metabolic SyndromekotraeNo ratings yet
- The Differences of Parathyroid Hormone, Vitamin D, and Calcium Ion Between Patients With Controlled and Uncontrolled Diabetes MellitusDocument4 pagesThe Differences of Parathyroid Hormone, Vitamin D, and Calcium Ion Between Patients With Controlled and Uncontrolled Diabetes MellitusErizal Dwi HandokoNo ratings yet
- Hyperlipidaemia in DiabetesDocument11 pagesHyperlipidaemia in Diabeteslakshminivas PingaliNo ratings yet
- 202-Article Text-345-1-10-20180117Document6 pages202-Article Text-345-1-10-20180117Fifi RetiatyNo ratings yet
- Vol 3 6 Sym9 Egi PDFDocument7 pagesVol 3 6 Sym9 Egi PDFCherryNo ratings yet
- Comparison OF Lipid Profile AND Antioxidant Enzymes Among South Indian MEN Consuming Coconut OIL AND Sunflower OILDocument7 pagesComparison OF Lipid Profile AND Antioxidant Enzymes Among South Indian MEN Consuming Coconut OIL AND Sunflower OILAdityaNo ratings yet
- 03 Irjcm 1 (4) Oa03 20160607 PDFDocument4 pages03 Irjcm 1 (4) Oa03 20160607 PDFbalthier37No ratings yet
- Heart Failure Medication Poster 2021 ESC4Document2 pagesHeart Failure Medication Poster 2021 ESC4rajkumarrajendramNo ratings yet
- ArticleDocument8 pagesArticlejbeezyNo ratings yet
- Biochemical and Hematological Parameters in ChroniDocument9 pagesBiochemical and Hematological Parameters in Chroniss solutionsNo ratings yet
- General Aspects of Diabetes Mellitus20160808 31394 U4lcrv With Cover Page v2Document13 pagesGeneral Aspects of Diabetes Mellitus20160808 31394 U4lcrv With Cover Page v2PanjiNo ratings yet
- Non-Alcoholic Fatty Liver DiseaseDocument35 pagesNon-Alcoholic Fatty Liver Diseaserigueiram100% (1)
- Uric Acid, The Metabolic Syndrome, and Renal DiseaseDocument4 pagesUric Acid, The Metabolic Syndrome, and Renal DiseaseraynanthaNo ratings yet
- Jurnal 4Document11 pagesJurnal 4Kholifatu UlfaNo ratings yet
- BIOS LIFE - Diabetes in Control Study #1 by Steven Freed and David JoffeDocument1 pageBIOS LIFE - Diabetes in Control Study #1 by Steven Freed and David JoffeHisWellnessNo ratings yet
- Lipid Profile and Antioxidant Enzymes in Coconut Oil ConsumersDocument4 pagesLipid Profile and Antioxidant Enzymes in Coconut Oil ConsumersPreethu AnuNo ratings yet
- Health20100700010 64690396Document5 pagesHealth20100700010 64690396MellTandiNo ratings yet
- Metabolites 10 00195 v2Document11 pagesMetabolites 10 00195 v2Aulia lestariNo ratings yet
- Disfuncion ErectilDocument3 pagesDisfuncion ErectilUrsula CaceresNo ratings yet
- Cardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Document34 pagesCardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Dee DNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- Statin RhabdoDocument18 pagesStatin RhabdoDismayana Anggita RostiNo ratings yet
- 2008 Article 50Document4 pages2008 Article 50danielmartinezNo ratings yet
- Research ArticleDocument11 pagesResearch ArticleWahyuniNo ratings yet
- CKD Research Menuscript Final AmiyanshuDocument11 pagesCKD Research Menuscript Final AmiyanshuAmiyanshu BeheraNo ratings yet
- Recalls of Compilation of Clinical ChemistryDocument10 pagesRecalls of Compilation of Clinical ChemistryDeniel BusiNo ratings yet
- Hepatic Steatosis DyslipidemiaDocument6 pagesHepatic Steatosis Dyslipidemiakarina nilasariNo ratings yet
- Metabolic Synd Dr. ToniDocument19 pagesMetabolic Synd Dr. ToniToni PinemNo ratings yet
- Neuropati DMDocument30 pagesNeuropati DMAnisa PutriNo ratings yet
- Vegter 2012 Sodium Intake Ace Inhibition and PRDocument9 pagesVegter 2012 Sodium Intake Ace Inhibition and PRwaji khanNo ratings yet
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialDocument4 pagesIntensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialSheebaNo ratings yet
- Pooja 6th Sem SeminarDocument21 pagesPooja 6th Sem Seminargaurav adhikariNo ratings yet
- Evaluation of Prediabetes in High Risk Population of Kashmir ValleyDocument5 pagesEvaluation of Prediabetes in High Risk Population of Kashmir ValleyIJAR JOURNALNo ratings yet
- Evaluation of Safety and Efficacy of Telmisartan-Amlodipine Combination in Treating HypertensionDocument13 pagesEvaluation of Safety and Efficacy of Telmisartan-Amlodipine Combination in Treating HypertensionMelanie BirthaharaNo ratings yet
- Chronic Kidney DiseaseDocument48 pagesChronic Kidney DiseaseDaniel Apuan SalviejoNo ratings yet
- Clinical Study Regarding The Effect of NDocument7 pagesClinical Study Regarding The Effect of NcolceardoinaNo ratings yet
- Síndrome MetabolicoDocument38 pagesSíndrome Metabolicogeard heizem gomez herediaNo ratings yet
- 2021 - Diab - The Efficacy and Safety of Novel Classes of Glucoselowering Drugs - MetanaliseDocument11 pages2021 - Diab - The Efficacy and Safety of Novel Classes of Glucoselowering Drugs - MetanaliseLuiz Fernando Fonseca VieiraNo ratings yet
- Correlation Between Fasting Blood Glucose and Hba1c With Vitamin D in Diabetes MellitusDocument4 pagesCorrelation Between Fasting Blood Glucose and Hba1c With Vitamin D in Diabetes MellitusErizal Dwi HandokoNo ratings yet
- Glucose Control in Diabetes: Focus On SulfhonylureaDocument93 pagesGlucose Control in Diabetes: Focus On SulfhonylureascribdNo ratings yet
- Association of Soluble Suppression of Tumorigenesis-2 (ST2) With Endothelial Function in Patients With Ischemic Heart FailureDocument11 pagesAssociation of Soluble Suppression of Tumorigenesis-2 (ST2) With Endothelial Function in Patients With Ischemic Heart Failurere septian IlhamsyahNo ratings yet
- 2011 - Denicola (Jurnal)Document9 pages2011 - Denicola (Jurnal)Riana HandayaniNo ratings yet
- Mental Health AwarenesDocument6 pagesMental Health AwarenesRiana HandayaniNo ratings yet
- Multiple Meaning Words: Grade 4 Vocabulary WorksheetDocument2 pagesMultiple Meaning Words: Grade 4 Vocabulary WorksheetRiana HandayaniNo ratings yet
- Prof DR DR Ariyanto Harsono Spa (K)Document63 pagesProf DR DR Ariyanto Harsono Spa (K)Riana HandayaniNo ratings yet
- FAQs On The Emergency Use Authorization For Remdesivir For Hospitalized COVID 10-01-20Document5 pagesFAQs On The Emergency Use Authorization For Remdesivir For Hospitalized COVID 10-01-20Riana HandayaniNo ratings yet
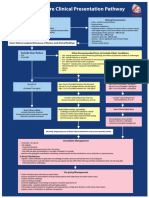
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- DigoxinDocument4 pagesDigoxinJaessa FelicianoNo ratings yet
- IANs Presentation - Atrial Fibrillation (RMO Kerenga)Document26 pagesIANs Presentation - Atrial Fibrillation (RMO Kerenga)Samuel.MoriNo ratings yet
- Pulseless Arrest Algorithm For Managing VF and Pulseless VTDocument3 pagesPulseless Arrest Algorithm For Managing VF and Pulseless VTLaili CinthiaNo ratings yet
- CAD NCP Decreased Cardiac OutputDocument3 pagesCAD NCP Decreased Cardiac OutputLeizel Apolonio100% (3)
- Guideline For The Evaluation and Management of Patients With SyncopeDocument99 pagesGuideline For The Evaluation and Management of Patients With SyncopePhúc Thiện NguyễnNo ratings yet
- VT Origin PDFDocument60 pagesVT Origin PDFNikita PratamaNo ratings yet
- ESC Congress 2020: The Digital ExperienceDocument9 pagesESC Congress 2020: The Digital ExperienceMeatus AcusticusNo ratings yet
- TachycardiaDocument12 pagesTachycardiaPuskesmas Pinang JayaNo ratings yet
- Surgical Management of Congenital Heart Disease II: Viktor Hraška Peter MurínDocument312 pagesSurgical Management of Congenital Heart Disease II: Viktor Hraška Peter MurínCardiologia PediatricaNo ratings yet
- Cardiogenic Pulmonary EdemaDocument1 pageCardiogenic Pulmonary EdemaAirish LimNo ratings yet
- Cardiovascular Drugs XL ChartDocument4 pagesCardiovascular Drugs XL Chartcdp158767% (3)
- ECG TerminologyDocument66 pagesECG TerminologyblndfflNo ratings yet
- Philippine Heart Center vs. Local Government of Quezon City GR No. 225409 11 March 2020.Document15 pagesPhilippine Heart Center vs. Local Government of Quezon City GR No. 225409 11 March 2020.TobyNo ratings yet
- Patient: Transthoracic Echocardiography ReportDocument2 pagesPatient: Transthoracic Echocardiography Reportluh sriaryantiNo ratings yet
- Iabp 3Document10 pagesIabp 3Diana Marcela Franco SanchezNo ratings yet
- ECG ArrhythmiaDocument27 pagesECG ArrhythmiaSrikitta DanieliaNo ratings yet
- Falso Tendão No VE e Repolarização VentricularDocument1 pageFalso Tendão No VE e Repolarização VentricularNITACORDEIRONo ratings yet
- AuscultationDocument41 pagesAuscultationAnonymous ZUaUz1wwNo ratings yet
- STRONG Fitness Magazine - 2014 - 01 Jan-Fev PDFDocument88 pagesSTRONG Fitness Magazine - 2014 - 01 Jan-Fev PDFJoana SoaresNo ratings yet
- BLS Aed ErcDocument34 pagesBLS Aed ErcNicoleta Pîrju100% (1)
- External Pulse Generator: Product HighlightsDocument2 pagesExternal Pulse Generator: Product HighlightsScrbdJoe100No ratings yet
- Bedside Cardiology (2012) (PDF)Document251 pagesBedside Cardiology (2012) (PDF)Loredana Dobrea100% (4)
- Sample: Analyzing The Heart With EKGDocument12 pagesSample: Analyzing The Heart With EKGJonathanNo ratings yet
- Desfibrilador, Mca. Zoll. Mod. PD 1400 - Manual Del OperadorDocument65 pagesDesfibrilador, Mca. Zoll. Mod. PD 1400 - Manual Del OperadorMiris RebollarNo ratings yet