You might also like
- High Prevalence of Proarrhythmic Events in PatientDocument8 pagesHigh Prevalence of Proarrhythmic Events in PatientAlda AdeliaNo ratings yet
- CirculatoryDocument13 pagesCirculatorysuelly-majorNo ratings yet
- Tebak AjaDocument3 pagesTebak AjaSanti P TambunanNo ratings yet
- Vasoplegia - Mechanism & Management Following CPB-1Document9 pagesVasoplegia - Mechanism & Management Following CPB-1somaraj kNo ratings yet
- Haas 2008Document4 pagesHaas 2008Ana CortezNo ratings yet
- The Heart Rate Response Pattern To Dialysis Hypotension in Haemodialysis PatientsDocument6 pagesThe Heart Rate Response Pattern To Dialysis Hypotension in Haemodialysis PatientsAnton SampNo ratings yet
- Bailey JMDocument9 pagesBailey JMPedro VillamorNo ratings yet
- Casos Medicina InternaDocument219 pagesCasos Medicina Internazara galiciaNo ratings yet
- Seizure Txa 1Document9 pagesSeizure Txa 1PeriUmardianaNo ratings yet
- The Heart Rate Response Pattern To Dialysis Hypotension in Haemodialysis PatientsDocument5 pagesThe Heart Rate Response Pattern To Dialysis Hypotension in Haemodialysis PatientsAnton SampNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Falla CardiacaDocument6 pagesFalla CardiacaFelipeNo ratings yet
- Anti ArrthymicDocument7 pagesAnti ArrthymicpvsvrNo ratings yet
- 2016 ESC Guidelines For The Diagnosis and Treatment of Acute Heart FailureDocument13 pages2016 ESC Guidelines For The Diagnosis and Treatment of Acute Heart FailurejoaoNo ratings yet
- ShockDocument16 pagesShockChristiaan VoslooNo ratings yet
- Aminas en ShockDocument14 pagesAminas en ShockRamón E. Reyes CáseresNo ratings yet
- European J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A ClinicalDocument12 pagesEuropean J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A ClinicalFerBullknockNo ratings yet
- Guide to perioperative management of pheochromocytomaDocument7 pagesGuide to perioperative management of pheochromocytomaamel melkiNo ratings yet
- Perianesthetic ArrhythmiasDocument10 pagesPerianesthetic Arrhythmiastaner_soysurenNo ratings yet
- Anesthetic Management of The Hypertensive Patient: Part II: Continuing Education in Honor of Norman Trieger, DMD, MDDocument8 pagesAnesthetic Management of The Hypertensive Patient: Part II: Continuing Education in Honor of Norman Trieger, DMD, MDFitri Aesthetic centerNo ratings yet
- Chronic Arrhythmia ManagementDocument44 pagesChronic Arrhythmia ManagementSulaiman TahsinNo ratings yet
- Low Cardiac Output ChildrenDocument11 pagesLow Cardiac Output ChildrenXavier AbrilNo ratings yet
- Inotropes 2014. Journal of The American College of CardiologyDocument10 pagesInotropes 2014. Journal of The American College of CardiologyFra1312No ratings yet
- BF03259831Document21 pagesBF03259831Punnaphat Tinnaphop DaraswangNo ratings yet
- touchCARDIO EJAE 7.1 pp04-11Document8 pagestouchCARDIO EJAE 7.1 pp04-11Carlos Navarro alonsoNo ratings yet
- AF DigoxinDocument13 pagesAF DigoxinDita NururiyanieNo ratings yet
- TilemahDocument7 pagesTilemahAndreea TudurachiNo ratings yet
- 12 CR Use of Tenecteplase For PDFDocument4 pages12 CR Use of Tenecteplase For PDFsameeNo ratings yet
- Anesthesia For An Adult Patient With Patent Ductus Arteriosus For Interval TubectomyDocument3 pagesAnesthesia For An Adult Patient With Patent Ductus Arteriosus For Interval TubectomyLalu Sohibul Rahman JNo ratings yet
- 1153-Article Text-4888-1-10-20200206 PDFDocument6 pages1153-Article Text-4888-1-10-20200206 PDFAdrian CaballesNo ratings yet
- Hemoragik TransformasiDocument5 pagesHemoragik TransformasiPPDS Neurologi USK 12No ratings yet
- 1993, EpsteinDocument5 pages1993, EpsteinRob AlexandersNo ratings yet
- Medip, IJAM-724 CDocument3 pagesMedip, IJAM-724 CKhalilSemlaliNo ratings yet
- 31-Article Text-56-1-10-20190118Document7 pages31-Article Text-56-1-10-20190118Fatos KatanolliNo ratings yet
- Vasopressors and Inotropes in ShockDocument8 pagesVasopressors and Inotropes in ShockRiska PashaNo ratings yet
- Cardioversion of Atrial Fibrillation and AtrialDocument13 pagesCardioversion of Atrial Fibrillation and AtrialLabontu IustinaNo ratings yet
- Hypothyroid CardiomyophathyDocument3 pagesHypothyroid Cardiomyophathysmartjohnsmith10No ratings yet
- Clinical Case Reports - 2020 - Schnaubelt - Hyperkalemia A Persisting Risk A Case Report and Update On Current ManagementDocument6 pagesClinical Case Reports - 2020 - Schnaubelt - Hyperkalemia A Persisting Risk A Case Report and Update On Current ManagementDesi MeliaNo ratings yet
- Af 1Document22 pagesAf 1muthiaraNo ratings yet
- Nathanson Et Al 1998 AnaesthesiaDocument12 pagesNathanson Et Al 1998 AnaesthesiaKetan HijauNo ratings yet
- Heart MurmurDocument6 pagesHeart MurmurYogendran MNo ratings yet
- Nursing in Critical Care - 2011 - Parry - Inotropic drugs and their uses in critical careDocument9 pagesNursing in Critical Care - 2011 - Parry - Inotropic drugs and their uses in critical careأركان هيلث Arkan healthNo ratings yet
- Cardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureDocument13 pagesCardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureGian CarloNo ratings yet
- 10 1016@j Amjcard 2015 01 455Document1 page10 1016@j Amjcard 2015 01 455Elis FatmayantiNo ratings yet
- Anesthetic Management of A Patient With Severe Systolic Dysfunction Posted For Proximal Femur Fracture Fixation - A Case ReportDocument2 pagesAnesthetic Management of A Patient With Severe Systolic Dysfunction Posted For Proximal Femur Fracture Fixation - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Managing Perioperative ArrhythmiasDocument15 pagesManaging Perioperative ArrhythmiasSudar Pecinta ParawaliNo ratings yet
- Sme PropofolDocument2 pagesSme PropofolAntonella Jazmín AssadNo ratings yet
- Targeting Cardiac Hypertrophy Toward A Causal.1Document13 pagesTargeting Cardiac Hypertrophy Toward A Causal.1Edith JeevanNo ratings yet
- 1.postoperative Arrhythmias After Cardiac SurgeryDocument16 pages1.postoperative Arrhythmias After Cardiac Surgeryganda gandaNo ratings yet
- Cardioembolic Stroke: Everything Has Changed: J David SpenceDocument8 pagesCardioembolic Stroke: Everything Has Changed: J David SpenceWaoNo ratings yet
- Atrial Fibrillation and Congestive Heart Failure: EditorialDocument3 pagesAtrial Fibrillation and Congestive Heart Failure: EditorialfederikarosilawatiNo ratings yet
- Restrictive Cardiomyopathy Associated With Long-Term Use of Hydroxychloroquine For Systemic Lupus ErythematosusDocument5 pagesRestrictive Cardiomyopathy Associated With Long-Term Use of Hydroxychloroquine For Systemic Lupus ErythematosusMichael GhattasNo ratings yet
- Anaesthetic Considerations for Mitral Valve ProlapseDocument7 pagesAnaesthetic Considerations for Mitral Valve ProlapsejaneelsenNo ratings yet
- European J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A ClinicalDocument12 pagesEuropean J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A Clinicalsomaraj kNo ratings yet
- Vasoplegic SyndromeDocument41 pagesVasoplegic SyndromeFaizan Ahmad Ali100% (1)
- The Use of Recombinant Factor Viia (Novoseven) For Treatment of Active or Impending Bleeding in Brain Injury: Broadening The IndicationsDocument7 pagesThe Use of Recombinant Factor Viia (Novoseven) For Treatment of Active or Impending Bleeding in Brain Injury: Broadening The IndicationsBig TexNo ratings yet
- Eisenmenger SyndromeDocument10 pagesEisenmenger SyndromeprastiaNo ratings yet
- Fibrilación AuricularDocument9 pagesFibrilación AuricularMartin De Santiago ValenzuelaNo ratings yet
- Fibrilacioni Atrial Trajtimi Dhe Diagnoza e TijDocument8 pagesFibrilacioni Atrial Trajtimi Dhe Diagnoza e TijMarsiano QendroNo ratings yet
- 1 s2.0 S0263931920302374 MainDocument7 pages1 s2.0 S0263931920302374 MainRakhmat RamadhaniNo ratings yet
- Neurorehabilitation TherapyDocument255 pagesNeurorehabilitation TherapyRakhmat RamadhaniNo ratings yet
- Antiplatelet Discontinuation Practices in CAD Patients Undergoing SurgeryDocument2 pagesAntiplatelet Discontinuation Practices in CAD Patients Undergoing SurgeryRakhmat RamadhaniNo ratings yet
- Effect of Aminophylline in CHB With Ventricular Asystole After Blunt Chest TraumaDocument4 pagesEffect of Aminophylline in CHB With Ventricular Asystole After Blunt Chest TraumaRakhmat RamadhaniNo ratings yet
- Adenosine Regulation of Immune Response Initiated in Ischemia Reperfusion InjuryDocument8 pagesAdenosine Regulation of Immune Response Initiated in Ischemia Reperfusion InjuryRakhmat RamadhaniNo ratings yet
- Advanced AV Block in Young and Middle Aged AdultsDocument11 pagesAdvanced AV Block in Young and Middle Aged AdultsRakhmat RamadhaniNo ratings yet
- Eletrefisiologia Da HipohipercalemiaDocument10 pagesEletrefisiologia Da HipohipercalemiaGabriel MouraNo ratings yet
- T Cell Immunity in Myocardial InflammationDocument12 pagesT Cell Immunity in Myocardial InflammationRakhmat RamadhaniNo ratings yet
- TR 2 138Document17 pagesTR 2 138Rakhmat RamadhaniNo ratings yet
- Socioeconomic Status and Mortality After Acute Myocardial Infarction: A Study From IranDocument10 pagesSocioeconomic Status and Mortality After Acute Myocardial Infarction: A Study From IranRakhmat RamadhaniNo ratings yet
- Jurnal-2-Naskah 3 JURNAL PDGI Vol 60 PDFDocument4 pagesJurnal-2-Naskah 3 JURNAL PDGI Vol 60 PDFSir_DebordesNo ratings yet
- Lappa, and Nigella Sativa: Article HistoryDocument8 pagesLappa, and Nigella Sativa: Article HistoryRakhmat RamadhaniNo ratings yet
- Evolution of Gray Zone After Acute Myocardial Infarction: Influence of Microvascular ObstructionDocument2 pagesEvolution of Gray Zone After Acute Myocardial Infarction: Influence of Microvascular ObstructionRakhmat RamadhaniNo ratings yet
- Strep EpidDocument8 pagesStrep EpidFhytria AraNo ratings yet
- 11-12 CSS Profile - Intl Students-Revised-20,000$Document4 pages11-12 CSS Profile - Intl Students-Revised-20,000$daubet84No ratings yet
- 11-12 CSS Profile - Intl Students-Revised-20,000$Document4 pages11-12 CSS Profile - Intl Students-Revised-20,000$daubet84No ratings yet
- PCM2014 - Sorin GroupDocument8 pagesPCM2014 - Sorin GroupDavid OrensteinNo ratings yet
- NR-TP-1211-037 - A3 - CN User Manual-Taurus PDFDocument117 pagesNR-TP-1211-037 - A3 - CN User Manual-Taurus PDFDamian RoweNo ratings yet
- Bioimplant Packaging - Nano TCDocument6 pagesBioimplant Packaging - Nano TCangelNo ratings yet
- US NCP-5 Owner Manual PN 21980-04 With Treatment Pants and Indications A PDFDocument103 pagesUS NCP-5 Owner Manual PN 21980-04 With Treatment Pants and Indications A PDFThanh Dao100% (1)
- Heart FailureDocument94 pagesHeart FailureAnusha Verghese100% (1)
- Bradycardia 1Document6 pagesBradycardia 1harasthaNo ratings yet
- Ecodrive 03Document44 pagesEcodrive 03Pablo OsoriaNo ratings yet
- SWDDocument58 pagesSWDakheel ahammedNo ratings yet
- ZOLL M2 Technical Specifications - ENDocument2 pagesZOLL M2 Technical Specifications - ENMuhammad SaadNo ratings yet
- Spring Term Core A Formative AssessmentDocument9 pagesSpring Term Core A Formative Assessmentdiscord.tazzNo ratings yet
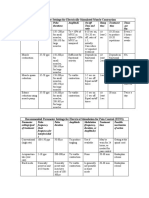
- Parameter Settings for Electrical StimulationDocument3 pagesParameter Settings for Electrical Stimulationpallen100% (5)
- Basics of PacemakerDocument121 pagesBasics of Pacemakerjeenath justin doss100% (1)
- Ibhre Prep 01 KeyDocument16 pagesIbhre Prep 01 Keyanon-747764100% (4)
- Desfibrilador - DefiMonitorXD - PRIMEDIC en InglesDocument74 pagesDesfibrilador - DefiMonitorXD - PRIMEDIC en Ingleserpadada100% (1)
- EP StudyDocument2 pagesEP StudyAdwait PatelNo ratings yet
- Prospekt Schiller ARGUS PRO LifeCare PDFDocument8 pagesProspekt Schiller ARGUS PRO LifeCare PDFFelix LeeNo ratings yet
- Pacemaker Implantation PowepointDocument15 pagesPacemaker Implantation Powepointapi-307732705No ratings yet
- Transcatheter Aortic Valve ImplantationDocument15 pagesTranscatheter Aortic Valve ImplantationJonathan BaileyNo ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- Valleylab Surgistat II User ManualDocument68 pagesValleylab Surgistat II User ManualFlatironsviewNo ratings yet
- Section 01 Be Plus Pro EngDocument105 pagesSection 01 Be Plus Pro EngTanzimul IslamNo ratings yet
- (Very Short Introductions) David Blockley - Engineering - A Very Short Introduction-Oxford University Press (2012)Document142 pages(Very Short Introductions) David Blockley - Engineering - A Very Short Introduction-Oxford University Press (2012)Khaled Sarhan100% (1)
- Samsung Gear 2 Sicherheitblatt PDFDocument760 pagesSamsung Gear 2 Sicherheitblatt PDFAnonymous 4Hm9h6ohdNo ratings yet
- Automotive recall numbers from 2006-2008Document435 pagesAutomotive recall numbers from 2006-2008nadeem hameedNo ratings yet
- LLDPE Dowlex 2645G TDSDocument3 pagesLLDPE Dowlex 2645G TDSAli RazuNo ratings yet
- Heart Dysrhythmias Cheat Sheet PDFDocument5 pagesHeart Dysrhythmias Cheat Sheet PDFbarbaraNo ratings yet
- Concord CPR ManualDocument54 pagesConcord CPR ManualtntranNo ratings yet
- LIFEPAK12 OperatingInstructions 3207254-008Document272 pagesLIFEPAK12 OperatingInstructions 3207254-008talunan23No ratings yet
- PacemakerDocument15 pagesPacemakermariet abraham100% (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)