You might also like
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Yuan2019 Article IronDeficiencyInLatePregnancyA PDFDocument11 pagesYuan2019 Article IronDeficiencyInLatePregnancyA PDFDekaraNo ratings yet
- Beta Vulgaris - Meningkatkan Level HBDocument4 pagesBeta Vulgaris - Meningkatkan Level HBReni WulansariNo ratings yet
- 90-Article Text-416-1-10-20201129Document4 pages90-Article Text-416-1-10-20201129Princess NavarroNo ratings yet
- Chand Yo 2015Document7 pagesChand Yo 2015Sakarias PanjaitanNo ratings yet
- Anemia in PregnancyDocument9 pagesAnemia in PregnancyShalini Shanmugalingam100% (1)
- Multiple Micronutrient Supplements During Pregnancy Do Not Reduce Anemia or Improve Iron Status Compared To Iron-Only Supplements in Semirural MexicoDocument14 pagesMultiple Micronutrient Supplements During Pregnancy Do Not Reduce Anemia or Improve Iron Status Compared To Iron-Only Supplements in Semirural MexicoRina ChairunnisaNo ratings yet
- Assessment of Dietary Pattern and Factors That Affect HemoglobinDocument7 pagesAssessment of Dietary Pattern and Factors That Affect HemoglobinJihan NurainiNo ratings yet
- Anemia and Iron Deficiency: Effects On Pregnancy Outcome: SupplementsDocument12 pagesAnemia and Iron Deficiency: Effects On Pregnancy Outcome: SupplementsLuis ChancusigNo ratings yet
- Iron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesDocument8 pagesIron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesAriyoko PatodingNo ratings yet
- Kriteria Rawat IcuDocument6 pagesKriteria Rawat Icuriska sovinaNo ratings yet
- Askeb JurnalDocument6 pagesAskeb JurnalUpi Krisdayanti LahaguNo ratings yet
- Refeeding Syndrome in The Neonatal Intensive Care Unit: JPPT - State of The Art ReviewDocument12 pagesRefeeding Syndrome in The Neonatal Intensive Care Unit: JPPT - State of The Art ReviewbacchiocchipaoloNo ratings yet
- Jurnal Anemia InternasionalDocument8 pagesJurnal Anemia InternasionalmeldhaNo ratings yet
- Iron Status and Risk Factors of Iron Deficiency Among Pregnant Women in Singapore A Cross-Sectional StudyDocument10 pagesIron Status and Risk Factors of Iron Deficiency Among Pregnant Women in Singapore A Cross-Sectional StudyMedical Record PPDS OBGINNo ratings yet
- Intervensi Suplemen Makanan Untuk Meningkatkan Kadar Hemoglobin Pada Ibu HamilDocument10 pagesIntervensi Suplemen Makanan Untuk Meningkatkan Kadar Hemoglobin Pada Ibu HamilArdysyah AriestyaNo ratings yet
- Medip,+433 1033 1 CEDocument5 pagesMedip,+433 1033 1 CESukma AuliaNo ratings yet
- 2 Pros. Nutrients-14-04091-V2Document10 pages2 Pros. Nutrients-14-04091-V2aliya kinantiNo ratings yet
- Nutrition: Previous Section Next SectionDocument11 pagesNutrition: Previous Section Next SectionAaliyaan KhanNo ratings yet
- s12884-020-03108-2Document8 pagess12884-020-03108-2Hanna 1253No ratings yet
- Serum Ferritin and Iron/TIBC of Pregnant Women Attending Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria: A Longitudinal StudyDocument6 pagesSerum Ferritin and Iron/TIBC of Pregnant Women Attending Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria: A Longitudinal StudyasclepiuspdfsNo ratings yet
- Tugas Inggris 3 Session 2Document221 pagesTugas Inggris 3 Session 2dinaNo ratings yet
- Jurnal Maya 1Document16 pagesJurnal Maya 1Azwad AnHty AsHty SlamanyaNo ratings yet
- Ijgo 14944Document9 pagesIjgo 14944onlydarkheartNo ratings yet
- Iron Supplementation and Physical Activity Lifestyle of Anaemic Pregnant WomenDocument14 pagesIron Supplementation and Physical Activity Lifestyle of Anaemic Pregnant Womennurul.kusumawardani nurul.kusumawardaniNo ratings yet
- HG Case StudyDocument12 pagesHG Case StudyleehiNo ratings yet
- BergenDocument13 pagesBergenElena VisterniceanNo ratings yet
- Prevalence of IDA among Pregnant Women in NablusDocument72 pagesPrevalence of IDA among Pregnant Women in NablusEArl CopinaNo ratings yet
- Temp FileDocument15 pagesTemp FileFerdous RezviNo ratings yet
- Does Effective Counseling Play An Important Role in Controlling Iron Deficiency Anemia Among Pregnant WomenDocument9 pagesDoes Effective Counseling Play An Important Role in Controlling Iron Deficiency Anemia Among Pregnant WomenAjay DNo ratings yet
- Effectiveness of Intravenous Iron Sucrose Versus Oral Iron in Iron Deficiency Anemia in PregnancyDocument9 pagesEffectiveness of Intravenous Iron Sucrose Versus Oral Iron in Iron Deficiency Anemia in PregnancyInternational Organization of Scientific Research (IOSR)No ratings yet
- Adherence To Iron Folate and Associated Factors Among Pregnant WomenDocument9 pagesAdherence To Iron Folate and Associated Factors Among Pregnant WomenBICARA JIWANo ratings yet
- Iron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesDocument8 pagesIron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesTenri Syahira SaidNo ratings yet
- Effect of Consuming Red Dragon Fruit (Hylocereus and Erythrocyte Among Pregnant WomenDocument10 pagesEffect of Consuming Red Dragon Fruit (Hylocereus and Erythrocyte Among Pregnant WomenIis MaisarohNo ratings yet
- CHAPTERSDocument22 pagesCHAPTERSArchana SahuNo ratings yet
- Ijrcog 13010oDocument5 pagesIjrcog 13010oEllen KopaNo ratings yet
- Kadar Feritin Serum Dan Hemoglobin Pada Wanita Pasangan Pengantin Baru Di BaliDocument5 pagesKadar Feritin Serum Dan Hemoglobin Pada Wanita Pasangan Pengantin Baru Di BaliRizq Felageti SNo ratings yet
- Iron and Folate SupplementationDocument6 pagesIron and Folate SupplementationDiaNo ratings yet
- BJH 9012Document13 pagesBJH 9012ooiziungieNo ratings yet
- Folic Acid Supplementation and Dietary Folate Intake Reduce Risk of PreeclampsiaDocument15 pagesFolic Acid Supplementation and Dietary Folate Intake Reduce Risk of PreeclampsiaDevi KharismawatiNo ratings yet
- The Change in Haemoglobin Concentration Between The First and Third Trimesters of Pregnancy: A Population StudyDocument6 pagesThe Change in Haemoglobin Concentration Between The First and Third Trimesters of Pregnancy: A Population Studymas nemoNo ratings yet
- Martial of Hypotrophe To Lubumbashi Factors Maternal Associated With Neonatal HypoferritinemiaDocument14 pagesMartial of Hypotrophe To Lubumbashi Factors Maternal Associated With Neonatal HypoferritinemiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptdessyevaNo ratings yet
- Zinc en Embarazo y Lactancia - 2012Document17 pagesZinc en Embarazo y Lactancia - 2012CHUri Ana CarlaNo ratings yet
- Iron Deficiency Anemia Among Preschooi Children (2-5) Years in Gaza StripDocument17 pagesIron Deficiency Anemia Among Preschooi Children (2-5) Years in Gaza StripMohammedAAl-HaddadAbo-alaaNo ratings yet
- UK Guidelines Iron Deficiency in Pregnancy PDFDocument34 pagesUK Guidelines Iron Deficiency in Pregnancy PDFYoga Rhamada SiregarNo ratings yet
- BMC Complementary and Alternative MedicineDocument8 pagesBMC Complementary and Alternative MedicineThiago NunesNo ratings yet
- 12 - 1 Annex 12Document18 pages12 - 1 Annex 12senadmt57No ratings yet
- Nutrients 12 01677Document14 pagesNutrients 12 01677Garvita KharbandaNo ratings yet
- Increased Hepcidin Levels in PreeclampsiaDocument7 pagesIncreased Hepcidin Levels in Preeclampsiaetwien reskintaNo ratings yet
- Commentary: Iron Deficiency of Pregnancy - A New Approach Involving Intravenous IronDocument7 pagesCommentary: Iron Deficiency of Pregnancy - A New Approach Involving Intravenous IronRaluca StaiculescuNo ratings yet
- Knowledge, Attitude and Practices of Pregnant Women Regarding Iron Deficiency Anemia in A Rural Area of LahoreDocument5 pagesKnowledge, Attitude and Practices of Pregnant Women Regarding Iron Deficiency Anemia in A Rural Area of Lahoreasthaq ahamedNo ratings yet
- Uk Guidelines Iron Deficiency in PregnancyDocument34 pagesUk Guidelines Iron Deficiency in PregnancyFirdaus AzinunNo ratings yet
- Comparative Study On Efficacy, Tolerability, and Cost of Different Iron Supplements Among Antenatal Women With Iron-Deficiency AnemiaDocument8 pagesComparative Study On Efficacy, Tolerability, and Cost of Different Iron Supplements Among Antenatal Women With Iron-Deficiency AnemiaAjay DNo ratings yet
- Effect of Consuming Red Dragon Fruit (Hylocereus Costaricensis) Juice On The Levels of Hemoglobin and Erythrocyte Among Pregnant Women PDFDocument10 pagesEffect of Consuming Red Dragon Fruit (Hylocereus Costaricensis) Juice On The Levels of Hemoglobin and Erythrocyte Among Pregnant Women PDFEndriany MaulaniNo ratings yet
- Effect of Consuming Red Dragon Fruit (Hylocereus Costaricensis) Juice On The Levels of Hemoglobin and Erythrocyte Among Pregnant WomenDocument10 pagesEffect of Consuming Red Dragon Fruit (Hylocereus Costaricensis) Juice On The Levels of Hemoglobin and Erythrocyte Among Pregnant WomenEndriany MaulaniNo ratings yet
- BHS InggrisDocument9 pagesBHS InggrisAies AishaNo ratings yet
- Implementasion TugasDocument8 pagesImplementasion TugasDetha NabutaekNo ratings yet
- Effect of iron, zinc, vitamin A supplements on Hb levels in pregnant womenDocument35 pagesEffect of iron, zinc, vitamin A supplements on Hb levels in pregnant womennovita yantiNo ratings yet
- Safety and Efficacy of Intravenous Iron Therapy in Postnatal Patients With Iron Deficiency AnemiaDocument4 pagesSafety and Efficacy of Intravenous Iron Therapy in Postnatal Patients With Iron Deficiency AnemiaJamatul FirdausNo ratings yet
- CH 15 QuizDocument8 pagesCH 15 QuizNelano EastNo ratings yet
- CIO Executive SummaryDocument8 pagesCIO Executive SummaryResumeBearNo ratings yet
- CW3 - 4Document2 pagesCW3 - 4Rigel Zabate100% (1)
- 125 128Document4 pages125 128Majdi JerbiNo ratings yet
- Instrument Landing SystemDocument35 pagesInstrument Landing SystemDena EugenioNo ratings yet
- Fatigue Analysis of Sundry I.C Engine Connecting Rods: SciencedirectDocument7 pagesFatigue Analysis of Sundry I.C Engine Connecting Rods: SciencedirectAshwin MisraNo ratings yet
- Instructions To Employee For Submitting Online Application For Transfer Under Rule - 38 of Postal Manual Vol.-IVDocument6 pagesInstructions To Employee For Submitting Online Application For Transfer Under Rule - 38 of Postal Manual Vol.-IVSankarMathi VaigundhamNo ratings yet
- Zodiac Working Boat MK6HDDocument4 pagesZodiac Working Boat MK6HDdan antonNo ratings yet
- Upliftment of Recto AveDocument6 pagesUpliftment of Recto AveFrance CortezanoNo ratings yet
- Task 7 Family Disaster Risk Reduction and Management PlanDocument7 pagesTask 7 Family Disaster Risk Reduction and Management PlanHaise SasakiNo ratings yet
- 11 - Surrogate Constraints 1968Document9 pages11 - Surrogate Constraints 1968asistensi pakNo ratings yet
- KEDIT User's GuideDocument294 pagesKEDIT User's GuidezamNo ratings yet
- Partial Full Volume of TankDocument8 pagesPartial Full Volume of TankBabita GuptaNo ratings yet
- Case Digest Basic Legal Ethics Subject FERDINAND A. CRUZ, Petitioner, vs. ALBERTO MINA, Et - Al., Respondents (G.R. No. 154207, 27 April 2007)Document3 pagesCase Digest Basic Legal Ethics Subject FERDINAND A. CRUZ, Petitioner, vs. ALBERTO MINA, Et - Al., Respondents (G.R. No. 154207, 27 April 2007)Grandeur P. G. GuerreroNo ratings yet
- Complete HSE document kit for ISO 14001 & ISO 45001 certificationDocument8 pagesComplete HSE document kit for ISO 14001 & ISO 45001 certificationfaroz khanNo ratings yet
- Ligot v. MathayDocument1 pageLigot v. MathayJoyce BaylonNo ratings yet
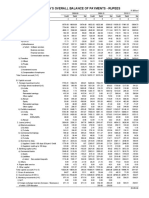
- Table 141: India'S Overall Balance of Payments - RupeesDocument2 pagesTable 141: India'S Overall Balance of Payments - Rupeesmahbobullah rahmaniNo ratings yet
- LuisRFlores (lf6225) UTRESUMEDocument3 pagesLuisRFlores (lf6225) UTRESUMELuis Rene FloresNo ratings yet
- HSD (1) .Product - Spec.sheet BootstrapReserviorDocument2 pagesHSD (1) .Product - Spec.sheet BootstrapReserviorJay R SVNo ratings yet
- Wa0031 PDFDocument1 pageWa0031 PDFAnaNo ratings yet
- Water Supply NED ArticleDocument22 pagesWater Supply NED Articlejulie1805No ratings yet
- As 2669-1983 Sulphuric Acid For Use in Lead-Acid BatteriesDocument7 pagesAs 2669-1983 Sulphuric Acid For Use in Lead-Acid BatteriesSAI Global - APACNo ratings yet
- Court Invalidates Mortgage Due to Bank's Lack of DiligenceDocument10 pagesCourt Invalidates Mortgage Due to Bank's Lack of DiligenceTokie TokiNo ratings yet
- Answer Key Determinants & Matrices: B C C B B C D A B CDocument2 pagesAnswer Key Determinants & Matrices: B C C B B C D A B CElbert EinsteinNo ratings yet
- Certificate of Analysis - Certified Reference Material: Cetyl PalmitateDocument6 pagesCertificate of Analysis - Certified Reference Material: Cetyl PalmitateRachel McArdleNo ratings yet
- Market Segmentation Targeting Strategy and Positioning Strategy Performance Effects To The Tourists Satisfaction Research in Pangandaran Beach Pangandaran DistrictDocument10 pagesMarket Segmentation Targeting Strategy and Positioning Strategy Performance Effects To The Tourists Satisfaction Research in Pangandaran Beach Pangandaran DistrictRizki Kurnia husainNo ratings yet
- Battery Calculations For Fire Alarm and Signaling SystemsDocument7 pagesBattery Calculations For Fire Alarm and Signaling Systemsleland macasinag100% (1)
- Sample BudgetDocument109 pagesSample BudgetAnjannette SantosNo ratings yet
- Un Authorised Sites Regularisation Within Sept 2009Document2 pagesUn Authorised Sites Regularisation Within Sept 2009Sridhara babu. N - ಶ್ರೀಧರ ಬಾಬು. ಎನ್No ratings yet
- Houghton Mifflin Harcourt Sap Document of UnderstandingDocument10 pagesHoughton Mifflin Harcourt Sap Document of UnderstandingSunil KumarNo ratings yet
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)From EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Rating: 4.5 out of 5 stars4.5/5 (52)
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingFrom EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingRating: 5 out of 5 stars5/5 (10)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionFrom EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionRating: 4.5 out of 5 stars4.5/5 (117)