You might also like
- Edmund Bergler - Divorce Won't HelpDocument256 pagesEdmund Bergler - Divorce Won't Helpbmx0100% (2)
- The Good News About Nuclear Destruction!Document7 pagesThe Good News About Nuclear Destruction!Ven GeanciaNo ratings yet
- Public Self-Perception, Knowledge and Practice About Covid-19 in Saudi ArabiaDocument11 pagesPublic Self-Perception, Knowledge and Practice About Covid-19 in Saudi ArabiaIJAR JOURNALNo ratings yet
- Knowledge, Attitude and Barriers Toward Covid-19 Vaccine Among Adults in Eastern Province, Kingdom of Saudi Arabia, 2021, Web-Based StudyDocument17 pagesKnowledge, Attitude and Barriers Toward Covid-19 Vaccine Among Adults in Eastern Province, Kingdom of Saudi Arabia, 2021, Web-Based StudyIJAR JOURNALNo ratings yet
- Aoun Et Al, 2021Document8 pagesAoun Et Al, 2021Oren KatzNo ratings yet
- Knowledge, Attitude and Practice About Covid-19 and Vaccine Acceptance Among Family Physician in Al-MadinahDocument9 pagesKnowledge, Attitude and Practice About Covid-19 and Vaccine Acceptance Among Family Physician in Al-MadinahIJAR JOURNALNo ratings yet
- Awareness and Perception of COVID-19 Among The General Population: A Middle Eastern SurveyDocument10 pagesAwareness and Perception of COVID-19 Among The General Population: A Middle Eastern SurveyManasi PandaNo ratings yet
- KAP2Document25 pagesKAP2mary ann masayonNo ratings yet
- Knowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointDocument6 pagesKnowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointAthenaeum Scientific PublishersNo ratings yet
- Knowledge and Attitudes Towards COVID-19 Vaccines Among University Students, Faculty Members and StaffsDocument9 pagesKnowledge and Attitudes Towards COVID-19 Vaccines Among University Students, Faculty Members and StaffsIJPHSNo ratings yet
- Knowledge, Attitude and Vaccination Status On Covid 19 Among Adults Living in Selected Rural Areas of Khurdha District, OdishaDocument6 pagesKnowledge, Attitude and Vaccination Status On Covid 19 Among Adults Living in Selected Rural Areas of Khurdha District, OdishaEditor IJTSRDNo ratings yet
- Knowledge, Attitude, Prevention Practice, and Associated Factors Toward COVID-19 Among Preparatory School Students in Southwest Ethiopia, 2021Document12 pagesKnowledge, Attitude, Prevention Practice, and Associated Factors Toward COVID-19 Among Preparatory School Students in Southwest Ethiopia, 2021DNo ratings yet
- A Review of Health Security and Vaccine Diplomacy During COVID-19 PandemicDocument8 pagesA Review of Health Security and Vaccine Diplomacy During COVID-19 PandemicIJPHSNo ratings yet
- HBM 1Document9 pagesHBM 1renzelpacleb123No ratings yet
- Level of Satisfaction With Covid-19 Vaccine After Getting Jabs Among The Generalpopulation in Gurgaon, HaryanaDocument7 pagesLevel of Satisfaction With Covid-19 Vaccine After Getting Jabs Among The Generalpopulation in Gurgaon, HaryanaIJAR JOURNALNo ratings yet
- Research Paper:: Health Responses During The COVID-19 Pandemic: An International Strategy and Experience AnalysisDocument14 pagesResearch Paper:: Health Responses During The COVID-19 Pandemic: An International Strategy and Experience AnalysisRobert BretonNo ratings yet
- Knowledge and Awareness Regarding Spread and Prevention of COVID-19 Among The Young Adults of KarachiDocument6 pagesKnowledge and Awareness Regarding Spread and Prevention of COVID-19 Among The Young Adults of KarachiWahyuni KarangNo ratings yet
- Ijcp 13891Document24 pagesIjcp 13891tugasdianok2No ratings yet
- Association Between Knowledge and Depression at Rising Time of COVID-19 in BangladeshDocument7 pagesAssociation Between Knowledge and Depression at Rising Time of COVID-19 in BangladeshIJPHSNo ratings yet
- The Relationship Between Age Groups and Knowledge and Understanding of Covid-19 VaccineDocument5 pagesThe Relationship Between Age Groups and Knowledge and Understanding of Covid-19 VaccineIJAR JOURNALNo ratings yet
- Community Voices Around COVID 19 Vaccine In.2Document11 pagesCommunity Voices Around COVID 19 Vaccine In.2Darshan GandhiNo ratings yet
- Covid 19Document7 pagesCovid 19Saurav KumarNo ratings yet
- Understanding COVID-19 Misinformation and Vaccine Hesitancy in Context - Findings From A Qualitative Study Involving Citizens in Bradford, UKDocument10 pagesUnderstanding COVID-19 Misinformation and Vaccine Hesitancy in Context - Findings From A Qualitative Study Involving Citizens in Bradford, UKMYNo ratings yet
- Acceptance and Attitudes Toward COVID-19 Vaccines: A Cross-Sectional Study From JordanDocument15 pagesAcceptance and Attitudes Toward COVID-19 Vaccines: A Cross-Sectional Study From JordanAmira SekrettNo ratings yet
- Journal Pone 0249716Document16 pagesJournal Pone 0249716Abhinaya A Saravanan UdayarNo ratings yet
- Article 2Document5 pagesArticle 2Ecnal JeremiahNo ratings yet
- Knowledge and Public Health Practices During Lockdown Towards COVID-19 in BangladeshDocument8 pagesKnowledge and Public Health Practices During Lockdown Towards COVID-19 in BangladeshIJPHSNo ratings yet
- Healthcare 11 00461 v2 PDFDocument13 pagesHealthcare 11 00461 v2 PDFFaye ToqueroNo ratings yet
- Ijst 2022 473Document6 pagesIjst 2022 473Sudharson KNo ratings yet
- Association of Individual Health Literacy With Preventive Behaviours and Family Well-Being During COVID-19 Pandemic - Mediating Role of Family Information Sharing.Document10 pagesAssociation of Individual Health Literacy With Preventive Behaviours and Family Well-Being During COVID-19 Pandemic - Mediating Role of Family Information Sharing.MYNo ratings yet
- Determinants of Covid 19 Vaccine Acceptance Shelden Kate C. PoyotDocument20 pagesDeterminants of Covid 19 Vaccine Acceptance Shelden Kate C. PoyotShelden KateNo ratings yet
- Factors Associated With post-COVID-19 ConfinementDocument1 pageFactors Associated With post-COVID-19 ConfinementRobby RanidoNo ratings yet
- Org ArabDocument13 pagesOrg Arabandros 77No ratings yet
- Knowledge, Attitude, and Practice Regarding COVID-19 Outbreak in Bangladesh: An Online-Based Cross-Sectional StudyDocument17 pagesKnowledge, Attitude, and Practice Regarding COVID-19 Outbreak in Bangladesh: An Online-Based Cross-Sectional StudyalodiarkNo ratings yet
- Knowledge and Perceptions On COVID 19 Among The University Students in Odisha An Online SurveyDocument4 pagesKnowledge and Perceptions On COVID 19 Among The University Students in Odisha An Online SurveyEditor IJTSRDNo ratings yet
- Knowledge, Precautionary Actions, and Perceived Risk of COVID-19 Among Indonesian PeopleDocument8 pagesKnowledge, Precautionary Actions, and Perceived Risk of COVID-19 Among Indonesian PeopleIJPHSNo ratings yet
- Ijerph 18 03804Document11 pagesIjerph 18 03804Gregorius Samuel GintingNo ratings yet
- Ijerph 18 03804Document11 pagesIjerph 18 03804Gregorius Samuel GintingNo ratings yet
- Soltan2020 Article KnowledgeRiskPerceptionAndPrevDocument8 pagesSoltan2020 Article KnowledgeRiskPerceptionAndPrevزينب بنت لفإل مدّسرNo ratings yet
- Perceived Risks of Infection Hospitalization and Death From Covid 19 at The Equator Ecuador and KenyaDocument17 pagesPerceived Risks of Infection Hospitalization and Death From Covid 19 at The Equator Ecuador and KenyaSiddharth JindalNo ratings yet
- Knowledge and Covid 19 Vaccine Uptake Among Elderly in Ogun State, NigeriaDocument7 pagesKnowledge and Covid 19 Vaccine Uptake Among Elderly in Ogun State, NigeriaInternational Journal of Innovative Science and Research Technology100% (1)
- Home Isolated COVID-19 Patients Adhering To Recommended Guidelines: A Cross Sectional Survey in KarachiDocument4 pagesHome Isolated COVID-19 Patients Adhering To Recommended Guidelines: A Cross Sectional Survey in KarachiFouzia ShariqNo ratings yet
- Jurnal BHS Inggris FixDocument10 pagesJurnal BHS Inggris FixadilaNo ratings yet
- Knowledge and Attitude Towards COVID-19 Among Adult People in Bangladesh: Evidence From An Online SurveyDocument11 pagesKnowledge and Attitude Towards COVID-19 Among Adult People in Bangladesh: Evidence From An Online SurveyIJPHSNo ratings yet
- 3rd R.LDocument14 pages3rd R.LWilliam Tac anNo ratings yet
- Factors Associated With COVID-19 Vaccine HesitancyDocument14 pagesFactors Associated With COVID-19 Vaccine HesitancyksmidhilaNo ratings yet
- Vacination ProgramDocument8 pagesVacination ProgramAlejandro Gabriel ArancibiaNo ratings yet
- Willingness To Pay-Magnamedika-Dr YuniDocument20 pagesWillingness To Pay-Magnamedika-Dr Yuninurmaulida568No ratings yet
- See ThroughDocument12 pagesSee ThroughAkash RahmanNo ratings yet
- Consciousness, Threats and Perceptions Towards Covid-19 Among The Business Persons of Agricultural Product Market, Birtamod, Jhapa, NepalDocument17 pagesConsciousness, Threats and Perceptions Towards Covid-19 Among The Business Persons of Agricultural Product Market, Birtamod, Jhapa, NepalAnonymous CwJeBCAXpNo ratings yet
- Factors Influencing Public Attitudes Towards COVID-19 Vaccination: A Scoping Review Informed by The Socio-Ecological ModelDocument27 pagesFactors Influencing Public Attitudes Towards COVID-19 Vaccination: A Scoping Review Informed by The Socio-Ecological ModelneneNo ratings yet
- DepressionDocument3 pagesDepressionemilpauloquibilanNo ratings yet
- Paper RemoladoDocument57 pagesPaper RemoladoJan Michael R. RemoladoNo ratings yet
- Students' Views On Vaccination Against COVID-19 Virus and Trust in Media Information About The Vaccine: The Case of SerbiaDocument13 pagesStudents' Views On Vaccination Against COVID-19 Virus and Trust in Media Information About The Vaccine: The Case of SerbiaRaven ShinNo ratings yet
- Attitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudyDocument7 pagesAttitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudydauntlessNo ratings yet
- Health Science Reports - 2022 - SeyedAlinaghi - Impact of COVID 19 Pandemic On Routine Vaccination Coverage of Children andDocument12 pagesHealth Science Reports - 2022 - SeyedAlinaghi - Impact of COVID 19 Pandemic On Routine Vaccination Coverage of Children andArumm88No ratings yet
- Awareness, Knowledge and TrustDocument15 pagesAwareness, Knowledge and TrustYosi Reskhiyani SimamoraNo ratings yet
- Pone 0236918Document13 pagesPone 0236918MegbaruNo ratings yet
- B12.Knowledge and Perceptions About COVID-19 Among The Medical and Allied Health Science Students in IndiaDocument6 pagesB12.Knowledge and Perceptions About COVID-19 Among The Medical and Allied Health Science Students in IndiaWislianaNo ratings yet
- An Investigation of The Association Between Religiouscoping Fatigue Anxiety and Depressive Symptoms During The COVID19 Pandemic in Moroccoa Webbased Crosssectional SurveyDocument13 pagesAn Investigation of The Association Between Religiouscoping Fatigue Anxiety and Depressive Symptoms During The COVID19 Pandemic in Moroccoa Webbased Crosssectional SurveySwati ParijaNo ratings yet
- Jurnal Hayyat Gempit SyakbanDocument12 pagesJurnal Hayyat Gempit SyakbanhayyatNo ratings yet
- COVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsFrom EverandCOVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsNo ratings yet
- Notification No.19151 - Revised Guidelines MUKTADocument22 pagesNotification No.19151 - Revised Guidelines MUKTADeepak PeraNo ratings yet
- MRM Minutes 2014Document7 pagesMRM Minutes 2014maheshNo ratings yet
- Superposition Principle, Repetitive IV, Drug Clearance (Sir Imran)Document21 pagesSuperposition Principle, Repetitive IV, Drug Clearance (Sir Imran)Rafay Sarwar MughalNo ratings yet
- Chinese GarterDocument3 pagesChinese Gartereden estrado mendoza100% (1)
- Communication and Nutrional EducationDocument11 pagesCommunication and Nutrional EducationSabrina PanjaitanNo ratings yet
- Traffic Signs ManualDocument334 pagesTraffic Signs Manualiwansalma100% (1)
- Staphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andDocument8 pagesStaphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andRisna IrvianiNo ratings yet
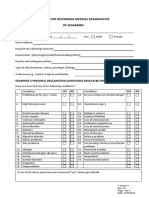
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Topic: Use of Antibiotic Therapy For Pediatric Dental PatientsDocument1 pageTopic: Use of Antibiotic Therapy For Pediatric Dental PatientsTenzin WangyalNo ratings yet
- Addison's DiseaseDocument17 pagesAddison's DiseaseMah Jezthy100% (1)
- Bioaviabality Bioequivalence 2nd Sem M.pharm PDFDocument10 pagesBioaviabality Bioequivalence 2nd Sem M.pharm PDFDipak bariNo ratings yet
- Vha Class III ListingDocument2,575 pagesVha Class III ListingpvenkyNo ratings yet
- Faradic: Reference ManualDocument19 pagesFaradic: Reference ManualrobertNo ratings yet
- Copd VS AsthmaDocument2 pagesCopd VS AsthmaHarkirat AtwalNo ratings yet
- (Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilDocument27 pages(Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilBrisa NarvaezNo ratings yet
- Lack of SleepDocument14 pagesLack of SleepBrigitta VianneyNo ratings yet
- Practice Essentials of Pulmonary ThromboembolismDocument39 pagesPractice Essentials of Pulmonary ThromboembolismEzzat Abdelhafeez SalemNo ratings yet
- 1P1 - Anna Kusumawati 323-329Document7 pages1P1 - Anna Kusumawati 323-329imam habibiNo ratings yet
- Jindal Steel SpecificationsDocument76 pagesJindal Steel SpecificationsVignesh Chellappan NatarajanNo ratings yet
- Milarchi Lara Bulletin - Monthi Fest Issue, September 2022Document52 pagesMilarchi Lara Bulletin - Monthi Fest Issue, September 2022Kemmannu comNo ratings yet
- Essay For TBIDocument7 pagesEssay For TBINatalie DrubachNo ratings yet
- Vol 19.1 - Sleep Disorders.2013Document252 pagesVol 19.1 - Sleep Disorders.2013Martoiu MariaNo ratings yet
- NHRA-PPR - Drug Price List - 06-10-2016Document595 pagesNHRA-PPR - Drug Price List - 06-10-2016Um AbdullaNo ratings yet
- Speaking AVCN2Document6 pagesSpeaking AVCN22253010690No ratings yet
- Daftar Obat Untuk Formularium KlinikDocument42 pagesDaftar Obat Untuk Formularium KlinikRianda LeeNo ratings yet
- The Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesDocument8 pagesThe Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesLwsynergylab OfficialNo ratings yet
- Department of Health v. C.V. Canchela & AssociatesDocument2 pagesDepartment of Health v. C.V. Canchela & AssociatesKelly RoxasNo ratings yet
- Kinjal AttachedDocument1 pageKinjal AttachedNilay JethavaNo ratings yet