You might also like
- Technology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementFrom EverandTechnology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementMichele FimianiNo ratings yet
- Hair LaserDocument10 pagesHair Laseriship pkmkenangaNo ratings yet
- Laser PsicosegundoDocument14 pagesLaser PsicosegundoCristiane RalloNo ratings yet
- M22 Plus 6 Page Brochure WEB PB 2000761 Rev B PDFDocument6 pagesM22 Plus 6 Page Brochure WEB PB 2000761 Rev B PDFali zeidNo ratings yet
- Laser Hair Removal (R. Anderson)Document14 pagesLaser Hair Removal (R. Anderson)Roxanne KapNo ratings yet
- PlatinumGMT Diode Laser - User Manual (Ver.3) (8519683)Document22 pagesPlatinumGMT Diode Laser - User Manual (Ver.3) (8519683)Lacramioara FituNo ratings yet
- Laser RX VADocument62 pagesLaser RX VAhaneefmdfNo ratings yet
- Roundtable Melasma TXDocument5 pagesRoundtable Melasma TXYulius67% (3)
- Laser Ndyag Canggih V12 ProDocument9 pagesLaser Ndyag Canggih V12 ProTigor ButarNo ratings yet
- Adss 1060nm Laser SculptureDocument10 pagesAdss 1060nm Laser SculptureAhmed OsmanNo ratings yet
- Harmony XL DR Bro PrintDocument16 pagesHarmony XL DR Bro PrintsilvioNo ratings yet
- Dynamic Cooling Device Laser Hair RemovalDocument10 pagesDynamic Cooling Device Laser Hair Removalshaktiman gangadharNo ratings yet
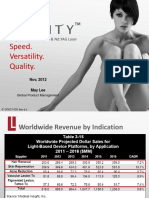
- Speed. Versatility. Quality.: Long Pulsed Alexandrite & Nd:YAG LaserDocument51 pagesSpeed. Versatility. Quality.: Long Pulsed Alexandrite & Nd:YAG LaserasdNo ratings yet
- Tag0708 Hairremchartv7-071708Document3 pagesTag0708 Hairremchartv7-071708yxmrsx100% (1)
- Tag0708 Vascularchartv7-071708Document3 pagesTag0708 Vascularchartv7-071708yxmrsxNo ratings yet
- Q - Switched LaserDocument54 pagesQ - Switched LaseralfanyNo ratings yet
- Focus. Flexibility. Freedom.: That's HarmonyDocument12 pagesFocus. Flexibility. Freedom.: That's HarmonyYohan WandishaNo ratings yet
- Evolution of Picosecond LaserDocument12 pagesEvolution of Picosecond Laserleenatalia93No ratings yet
- Clinical Training GuideDocument33 pagesClinical Training GuideJose GuzmanNo ratings yet
- Shr-Ipl-Rf BalanceDocument37 pagesShr-Ipl-Rf BalancerudavanegasNo ratings yet
- Electro-Optical Synergy (ELOS) Technology For Combined Acne Scars PDFDocument4 pagesElectro-Optical Synergy (ELOS) Technology For Combined Acne Scars PDFAryantii AntyNo ratings yet
- Yag Laser Tattoo Removal: User'S Manual MODEL: Yinhe-V18 UserDocument18 pagesYag Laser Tattoo Removal: User'S Manual MODEL: Yinhe-V18 Usersec.ivbNo ratings yet
- Technical Users Manual Fraxel Re Store DUAL Wavelength SystemDocument80 pagesTechnical Users Manual Fraxel Re Store DUAL Wavelength SystemCamila LopezNo ratings yet
- Lumenis - M22 - Before and After Case Book PDFDocument28 pagesLumenis - M22 - Before and After Case Book PDFPatrick Kim100% (1)
- Unmatched Nd:Yag Technology: SpecificationsDocument2 pagesUnmatched Nd:Yag Technology: SpecificationsAndrea MejiaNo ratings yet
- Ipl BeautyDocument40 pagesIpl BeautydahonoNo ratings yet
- Gentlemax Pro: Integrated Aesthetic Treatment SystemDocument7 pagesGentlemax Pro: Integrated Aesthetic Treatment SystemAsmaa MostafaNo ratings yet
- A Review of The Adverse Effects of Laser Hair RemovalDocument5 pagesA Review of The Adverse Effects of Laser Hair RemovalSimão NóbregaNo ratings yet
- Hair Removal by Forma™ IPL System, Study of Efficiency and Side EffectsDocument2 pagesHair Removal by Forma™ IPL System, Study of Efficiency and Side EffectsSoraya Eva EffridzaNo ratings yet
- FDA SofwaveDocument9 pagesFDA SofwavePhúc LâmNo ratings yet
- Type of Device Indications and Usage: X-Ray Uv Visible InfraredDocument8 pagesType of Device Indications and Usage: X-Ray Uv Visible InfraredErica Conner Menendez100% (1)
- Lasers in Dermatological Practice PDF UnitedvrgDocument574 pagesLasers in Dermatological Practice PDF Unitedvrgблогер бро100% (1)
- Co2 Laser CatalogueDocument24 pagesCo2 Laser CatalogueBlin RodsNo ratings yet
- Hifu 3d-1Document6 pagesHifu 3d-1sadraNo ratings yet
- opt manual - 纯白Document22 pagesopt manual - 纯白Seleccion HumanosNo ratings yet
- Nordlys™ Candela MedicalDocument1 pageNordlys™ Candela MedicalIsmaelNo ratings yet
- UntitledDocument30 pagesUntitledLee LeeNo ratings yet
- Jett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFDocument27 pagesJett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFMichaely Natali100% (1)
- Thulium Fiber Laser The New Player For Kidney Stone TreatmentDocument12 pagesThulium Fiber Laser The New Player For Kidney Stone TreatmentdrunkpunchloveNo ratings yet
- Clinical Guide - Diode LaserDocument7 pagesClinical Guide - Diode LaserPatricia Fernanda Lagos Cáceres100% (1)
- TN-1-IPL Applicators Modification and New Supporting Software VersionsDocument4 pagesTN-1-IPL Applicators Modification and New Supporting Software VersionsHill WnagNo ratings yet
- Document 3a1000052797Document13 pagesDocument 3a1000052797DolgarmoniNo ratings yet
- 蓝壳 Tattoo RemvoalDocument12 pages蓝壳 Tattoo RemvoalJorgeNo ratings yet
- Manual Mychway Equipo EsteticaDocument10 pagesManual Mychway Equipo EsteticaCata GodoyNo ratings yet
- Desktop User ManualDocument33 pagesDesktop User ManualJorge CoboNo ratings yet
- Soprano Laser User Manual (1600w+1600w)Document15 pagesSoprano Laser User Manual (1600w+1600w)SkinFudge ClinicsNo ratings yet
- Candela CO2Re BRDocument8 pagesCandela CO2Re BRAlex ZPNo ratings yet
- Laser Hair Removal GuidelinesDocument28 pagesLaser Hair Removal GuidelinesMIKENo ratings yet
- Fotona Dentistry BrochureDocument12 pagesFotona Dentistry BrochureiuliaNo ratings yet
- Fractional CO2 Laser Treatment For StretchmarksDocument6 pagesFractional CO2 Laser Treatment For StretchmarksShinagawaPh Main100% (1)
- Laser Therapy and Photosensitive MedicationDocument4 pagesLaser Therapy and Photosensitive MedicationEduardo Garza GarzaNo ratings yet
- Treat Any Age and Any Skin Type With Outstanding Results: AestheticDocument8 pagesTreat Any Age and Any Skin Type With Outstanding Results: AestheticEvelinaNo ratings yet
- Carbon Facial Copies of SlidesDocument33 pagesCarbon Facial Copies of Slides77yr72cdh6No ratings yet
- Portable IPL RF User ManualDocument22 pagesPortable IPL RF User Manualdahono100% (1)
- Manual Fotona Fidelis Plus II CE ENGDocument63 pagesManual Fotona Fidelis Plus II CE ENGблогер бро100% (1)
- Eagau08 Acnechartv6-090208Document2 pagesEagau08 Acnechartv6-090208yxmrsxNo ratings yet
- MOTUS AX - Clinical Manual Rev 2-0Document36 pagesMOTUS AX - Clinical Manual Rev 2-0محمد سامىNo ratings yet
- YH-5504SB ManualDocument17 pagesYH-5504SB ManualBill BrownNo ratings yet
- Laser Lipolysis: An UpdateDocument10 pagesLaser Lipolysis: An UpdateJamesNo ratings yet
- Tales From The Thousand and One NightsDocument98 pagesTales From The Thousand and One Nights_ele_mentalNo ratings yet
- Physical Description Fun Activities Games - 59525Document26 pagesPhysical Description Fun Activities Games - 59525_ele_mentalNo ratings yet
- Answer Key Dictation Task 6Document1 pageAnswer Key Dictation Task 6_ele_mentalNo ratings yet
- Miami Police File The O'Nell CaseDocument98 pagesMiami Police File The O'Nell CaseBelisario Marquez100% (1)
- The Diamond As Big As The Ritz by F. Scott FitzgeraldDocument98 pagesThe Diamond As Big As The Ritz by F. Scott Fitzgerald_ele_mentalNo ratings yet
- The Hound of The Baskervilles by Sir Arthur Conan DoyleDocument114 pagesThe Hound of The Baskervilles by Sir Arthur Conan Doyle_ele_mental100% (1)
- Moonfleet by John Meade FalknerDocument113 pagesMoonfleet by John Meade Falkner_ele_mental100% (2)
- Home For Christmas by Andrea M. HutchinsonDocument82 pagesHome For Christmas by Andrea M. Hutchinson_ele_mental100% (1)
- Three Men in A Boat PDFDocument113 pagesThree Men in A Boat PDFvalentina kovalesky100% (3)
- Lord Arthur Savile's Crime and Other Stories by Oscar WildeDocument114 pagesLord Arthur Savile's Crime and Other Stories by Oscar Wilde_ele_mental100% (1)
- Conan Doyle Arthur Sherlock Holmes StoriesDocument98 pagesConan Doyle Arthur Sherlock Holmes Stories_ele_mental100% (4)
- 06 SyntaxDocument14 pages06 SyntaxFatiFlureNo ratings yet
- The Prisoner of ZendaDocument130 pagesThe Prisoner of Zenda_ele_mental100% (1)
- KimDocument129 pagesKimfasakilasNo ratings yet
- Lista de Juegos Compatibles Con FreedomDocument47 pagesLista de Juegos Compatibles Con FreedomJuan Valentin33% (12)
- The Real McCoy and Other Ghost StoriesDocument24 pagesThe Real McCoy and Other Ghost Stories_ele_mentalNo ratings yet
- Missing in Sydney by Andrea M. HutchitsonDocument82 pagesMissing in Sydney by Andrea M. Hutchitson_ele_mental100% (1)
- Laser Tattoo RemovalDocument13 pagesLaser Tattoo RemovalAnonymous GUXjVMXUNo ratings yet
- Evolution of Picosecond LaserDocument12 pagesEvolution of Picosecond Laserleenatalia93No ratings yet
- Soprano Laser Consent FormDocument7 pagesSoprano Laser Consent FormBrianZack100% (1)
- Picocare 450 BrochureDocument2 pagesPicocare 450 Brochureammar hamzehNo ratings yet
- Remove Your Body Hair by Laser Hair Removal Method - OtdDocument2 pagesRemove Your Body Hair by Laser Hair Removal Method - OtdPunarnawah ClinicNo ratings yet
- AESTHETICS LASER PORTFOLIO - Quanta System - PDF Catalogs - Technical DocumentationDocument7 pagesAESTHETICS LASER PORTFOLIO - Quanta System - PDF Catalogs - Technical DocumentationMunir AldeekNo ratings yet
- Cometic ArticleDocument7 pagesCometic Articlevipul mahajanNo ratings yet
- Picosecond User ManualDocument32 pagesPicosecond User Manualjulio cesar torres vanegasNo ratings yet
- LaserDocument55 pagesLaserwalid_mohammady1616No ratings yet
- Laser Tattoo Removal A Clinical UpdateDocument7 pagesLaser Tattoo Removal A Clinical UpdateNur Alisya Hasnul HadiNo ratings yet
- Research 2Document29 pagesResearch 2Brenda EncarnacionNo ratings yet
- Xeo TreatmentsDocument13 pagesXeo TreatmentsSimone WallisNo ratings yet
- Plastic Surgery Exam Questions and Answers1 PDFDocument468 pagesPlastic Surgery Exam Questions and Answers1 PDFFeliciaDewi100% (1)
- Annual Book 13-14Document151 pagesAnnual Book 13-14Anshul VarshneyNo ratings yet
- Epl500 3 in 1 Ipl SHR Yag RF Catalgoe 20180206Document10 pagesEpl500 3 in 1 Ipl SHR Yag RF Catalgoe 20180206Anisia StefanNo ratings yet
- ADSS CatalogueDocument28 pagesADSS CataloguelenaNo ratings yet
- Adolescent and Young Adult TattooingDocument18 pagesAdolescent and Young Adult TattooingsergioNo ratings yet
- Picosecond User ManualDocument27 pagesPicosecond User Manualbasel zakiNo ratings yet
- CynosureDocument32 pagesCynosureJoseph DanielNo ratings yet
- TatooDocument100 pagesTatooSérgio Rohden100% (1)
- KATALOG RSI JULI 2020 Update 25 Juli 2020 PDFDocument35 pagesKATALOG RSI JULI 2020 Update 25 Juli 2020 PDFYulia HermansyahNo ratings yet
- Tattoo MagazineDocument36 pagesTattoo MagazineHannah CurryNo ratings yet
- Bcs Aesthetics Profile - ZapDocument25 pagesBcs Aesthetics Profile - ZapAmelluves ImanNo ratings yet
- Q - SWITCH - Starwalker - v4 - Fotona - July - 17 - AppDocument20 pagesQ - SWITCH - Starwalker - v4 - Fotona - July - 17 - Appmedhat fathyNo ratings yet
- EnglezaDocument16 pagesEnglezaAndreas SalajanNo ratings yet
- PU00992EN Rev A - PicoWay Medical Sell Sheet - LRDocument2 pagesPU00992EN Rev A - PicoWay Medical Sell Sheet - LRhadeer mahmoudNo ratings yet
- 06 DR Abraham Arimuko - Laser Co2 OverviewDocument35 pages06 DR Abraham Arimuko - Laser Co2 OverviewJohanna NathasiaNo ratings yet
- PB86102EN RevC PicoWay Product Brochure-LRDocument8 pagesPB86102EN RevC PicoWay Product Brochure-LRhadeer mahmoudNo ratings yet
- Carbon Facial Copies of SlidesDocument33 pagesCarbon Facial Copies of Slides77yr72cdh6No ratings yet
- Rethinking The Art of Tattoo: A Perspective of Indonesian Women Tattoo CommunityDocument11 pagesRethinking The Art of Tattoo: A Perspective of Indonesian Women Tattoo CommunityZulfikar Rachman100% (1)