You might also like
- Lecture 6 Breach Presentation Transversal Oblique LieDocument51 pagesLecture 6 Breach Presentation Transversal Oblique Lietanmai nooluNo ratings yet
- Anatomi Fisiologi KorneaDocument11 pagesAnatomi Fisiologi KorneaMauVeeNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- REVIEWCOURSEDocument102 pagesREVIEWCOURSEAjay KhadkaNo ratings yet
- Riau Nursing Conference 2020Document100 pagesRiau Nursing Conference 2020Junaidy Suparman RustamNo ratings yet
- Informe de Laboratorio No1Document50 pagesInforme de Laboratorio No1Alexsandro BonillaNo ratings yet
- SepsisDocument16 pagesSepsisDaniela100% (1)
- Kuliah GastroDocument119 pagesKuliah GastroMonazzt AsshagabNo ratings yet
- Kasus Hernia InguinalisDocument20 pagesKasus Hernia InguinalisAliyah rezky FahiraNo ratings yet
- AppenDocument54 pagesAppenmoqtadirNo ratings yet
- Total Mesorectal Excision (Tme)Document19 pagesTotal Mesorectal Excision (Tme)Mehtab JameelNo ratings yet
- Intraoperative Posterior Polar Cortical Disc.Document5 pagesIntraoperative Posterior Polar Cortical Disc.Danty IndriastutyNo ratings yet
- Pterigium: Dr. Purnamanita Syawal, SPM, MarsDocument39 pagesPterigium: Dr. Purnamanita Syawal, SPM, Marsyayat muhammadNo ratings yet
- Ahmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraDocument79 pagesAhmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraTekkhapulephel ParidudinNo ratings yet
- 6 MIKROTIA Ade - Unpad Full TextDocument23 pages6 MIKROTIA Ade - Unpad Full TextfakhrenaNo ratings yet
- Salman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Document459 pagesSalman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Silvia SanduNo ratings yet
- ColonosDocument8 pagesColonosHengki YongNo ratings yet
- MK Giz Slide Malnutrisi Energi ProteinDocument88 pagesMK Giz Slide Malnutrisi Energi ProteinAri AndryNo ratings yet
- Middle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDDocument66 pagesMiddle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDyusnafratilova16No ratings yet
- Factors Related to Medication Adherence in Schizophrenia PatientsDocument14 pagesFactors Related to Medication Adherence in Schizophrenia PatientsArvinae NovieNo ratings yet
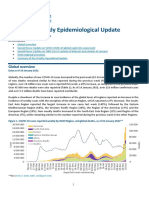
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument16 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewElia Nur IrmantiNo ratings yet
- Introduction To Clinical Radiology: The Breast: Priscilla J. Slanetz MD, MPH Assistant Professor of RadiologyDocument10 pagesIntroduction To Clinical Radiology: The Breast: Priscilla J. Slanetz MD, MPH Assistant Professor of Radiologydrqazi777No ratings yet
- Classification of CataractsDocument8 pagesClassification of CataractsAbdelrahman M. AlnweiriNo ratings yet
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- Thoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryDocument8 pagesThoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryIJAR JOURNALNo ratings yet
- AAO Glaucoma 2018Document87 pagesAAO Glaucoma 2018ismkipendprowil2No ratings yet
- NBSS AIA - Ivan Christian ChannelDocument128 pagesNBSS AIA - Ivan Christian ChannelASTAGINA NAURAHNo ratings yet
- Kuliah EmergensiDocument66 pagesKuliah EmergensiRifqi RamdhaniNo ratings yet
- Krisis MGDocument41 pagesKrisis MGasriNo ratings yet
- Feeding Jejunostomy and Ileostomy ChoicesDocument4 pagesFeeding Jejunostomy and Ileostomy ChoicesFikranaya SalimNo ratings yet
- Uroflowmetry InterpretationDocument4 pagesUroflowmetry InterpretationMeryl PulcheriaNo ratings yet
- Risk Stratification Algorithm For Orthopaedic Trauma Patients at Risk For Fat EmbolismDocument43 pagesRisk Stratification Algorithm For Orthopaedic Trauma Patients at Risk For Fat EmbolismAravind RaviNo ratings yet
- Limbal DermoidDocument4 pagesLimbal DermoidPranjali ChhayaNo ratings yet
- 42fundus AngiographyDocument28 pages42fundus AngiographyHitesh SharmaNo ratings yet
- Post Partum Hemorrhage 1Document41 pagesPost Partum Hemorrhage 1LineNo ratings yet
- Radiology of The AbdomenDocument19 pagesRadiology of The AbdomenShaktisila FatrahadyNo ratings yet
- Bowel ObstructionDocument48 pagesBowel ObstructionItHa Sagiitariius BLue LoverzNo ratings yet
- Anatomy, Embryology and Uterine AnomailesDocument45 pagesAnatomy, Embryology and Uterine AnomailesMesk BanatNo ratings yet
- Case Report: Urine Retention Et Causa Benign Hyperplasia ProstatDocument37 pagesCase Report: Urine Retention Et Causa Benign Hyperplasia ProstatKania A BustamNo ratings yet
- Aquas Humor DynamicsDocument30 pagesAquas Humor DynamicsRatnesh ShuklaNo ratings yet
- Open Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialDocument7 pagesOpen Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialAthenaeum Scientific PublishersNo ratings yet
- Pang ExpansionSphincter PDFDocument70 pagesPang ExpansionSphincter PDFIñaki ErdozáinNo ratings yet
- Guide to Intraocular Cataract Extraction Techniques (ICCE ECCEDocument61 pagesGuide to Intraocular Cataract Extraction Techniques (ICCE ECCEBboy ToonNo ratings yet
- S31 Wood S Light in DermatologyDocument8 pagesS31 Wood S Light in DermatologyGabriel CampolinaNo ratings yet
- DEPKES Pedoman Nasional Penanggulangan TBC 201Document113 pagesDEPKES Pedoman Nasional Penanggulangan TBC 201sugiarto M To'aNo ratings yet
- Visualize Lymphatic System Using X-Rays (LymphographyDocument11 pagesVisualize Lymphatic System Using X-Rays (LymphographyPax Giuseppe0% (1)
- ENLS Sub-Arachnoid Hemorrhage ProtocolDocument22 pagesENLS Sub-Arachnoid Hemorrhage ProtocolFransiskus MikaelNo ratings yet
- Pembahasan CBT COMBO 3Document802 pagesPembahasan CBT COMBO 3Sari Dewi WiratsihNo ratings yet
- Jaundice: Slide 001Document91 pagesJaundice: Slide 001mel_napsterNo ratings yet
- Blighted Ovum PDFDocument4 pagesBlighted Ovum PDFGopurS100% (1)
- The Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFDocument5 pagesThe Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFAsrori AzharNo ratings yet
- DrusenDocument34 pagesDrusendrunnibamsNo ratings yet
- MCU Analysis Indolakto Purwosari 2017Document102 pagesMCU Analysis Indolakto Purwosari 2017Ririn WidyaNo ratings yet
- PHD Seminar (Oral Cancer) (Prasad Rathod)Document31 pagesPHD Seminar (Oral Cancer) (Prasad Rathod)Apurv SoniNo ratings yet
- Diagnosis and Management of Infantile HemangiomaDocument47 pagesDiagnosis and Management of Infantile HemangiomaSteph FergusonNo ratings yet
- European Association of Urology Guideline 2018 PDFDocument1,268 pagesEuropean Association of Urology Guideline 2018 PDFMik WishNo ratings yet
- Suprapubic CathetherisationDocument33 pagesSuprapubic CathetherisationWahyuWNo ratings yet
- Transoral Laser Surgery For Supraglottic CancerDocument9 pagesTransoral Laser Surgery For Supraglottic CancerJose ManuelNo ratings yet
- Laparoscopic Resection of Rectal CancerDocument4 pagesLaparoscopic Resection of Rectal CancerhoangducnamNo ratings yet
- Colonic Interposition For Benign DiseaseDocument18 pagesColonic Interposition For Benign DiseaseOhana S.No ratings yet
- 10.1038@s41585 019 0212 4Document21 pages10.1038@s41585 019 0212 4Ohana S.No ratings yet
- Control of Bleeding From The Portal-Superior Mesenteric VeinDocument8 pagesControl of Bleeding From The Portal-Superior Mesenteric VeinOhana S.No ratings yet
- Complex Hepatic InjuriesDocument15 pagesComplex Hepatic InjuriesOhana S.No ratings yet
- Component Separation Technique To Repair Large Midline HerniasDocument10 pagesComponent Separation Technique To Repair Large Midline HerniasOhana S.No ratings yet
- Bladder and Ureteral InjuriesDocument13 pagesBladder and Ureteral InjuriesOhana S.No ratings yet
- Conventional and Laparoscopic Epigastric Hernia RepairDocument4 pagesConventional and Laparoscopic Epigastric Hernia RepairOhana S.No ratings yet
- CholedochoduodenostomyDocument7 pagesCholedochoduodenostomyOhana S.No ratings yet
- Diseccion Axilar-1Document15 pagesDiseccion Axilar-1Angelo DollyNo ratings yet
- Abdominoperineal ResectionDocument17 pagesAbdominoperineal ResectionOhana S.No ratings yet
- Closure of Duodenal PerforationsDocument6 pagesClosure of Duodenal PerforationsOhana S.No ratings yet
- AntrectomyDocument15 pagesAntrectomyOhana S.No ratings yet
- Goel - 1994 - Plate and Screw Fixation For Atlanto-Axial SubluxationDocument7 pagesGoel - 1994 - Plate and Screw Fixation For Atlanto-Axial SubluxationOhana S.No ratings yet
- Exalt HimDocument2 pagesExalt HimSaxon Inga100% (1)
- B. Wordsworth by V.S. NaipaulDocument18 pagesB. Wordsworth by V.S. NaipaulanushkahazraNo ratings yet
- Harry Potter Essay 1 OutlineDocument10 pagesHarry Potter Essay 1 OutlinevickaduzerNo ratings yet
- BadjaoDocument3 pagesBadjaochristianpauloNo ratings yet
- Two Contributions To The Foundations of Set TheoryDocument9 pagesTwo Contributions To The Foundations of Set TheoryDietethiqueNo ratings yet
- Arsenic and Old LaceDocument180 pagesArsenic and Old LaceGlenn Calvin50% (2)
- MIL PretestDocument1 pageMIL PretestAbram John Cabrales AlontagaNo ratings yet
- Curriculum Vitae: About MyselfDocument5 pagesCurriculum Vitae: About MyselfRahat Singh KachhwahaNo ratings yet
- Concrete Mix DesignDocument21 pagesConcrete Mix DesignIftikhar KamranNo ratings yet
- Marketing Plan For RESUVADocument31 pagesMarketing Plan For RESUVAMohammad Shaniaz Islam75% (4)
- Design and Construction of A Wireless We PDFDocument69 pagesDesign and Construction of A Wireless We PDFPeculiar EbhueleNo ratings yet
- Kinetic Study of Crystal Violet ReactionDocument10 pagesKinetic Study of Crystal Violet ReactionTaniya GuptaNo ratings yet
- Conversation LaundryDocument2 pagesConversation Laundryvanni octavania88% (8)
- Reaction KineticsDocument37 pagesReaction KineticsDaisyNo ratings yet
- The Path To Dignity and Respect enDocument73 pagesThe Path To Dignity and Respect enStan BuddenNo ratings yet
- 2020 CPS Kindergarten Readiness StudyDocument31 pages2020 CPS Kindergarten Readiness StudyCincinnatiEnquirerNo ratings yet
- Alliance of Nationalist and Genuine Labor Org Vs Samahan NG Mga Mangagawang Nagkakaisa Sa Manila Bay Spinning MillsDocument8 pagesAlliance of Nationalist and Genuine Labor Org Vs Samahan NG Mga Mangagawang Nagkakaisa Sa Manila Bay Spinning MillspasmoNo ratings yet
- Crime Trend CompletedDocument15 pagesCrime Trend CompletedLENARD LAGASINo ratings yet
- BSBPMG522 assessment tasksDocument30 pagesBSBPMG522 assessment tasksPokemon Legend0% (1)
- AnticoagulantsDocument19 pagesAnticoagulantsOsama ZbedaNo ratings yet
- Engro HRMDocument31 pagesEngro HRMtommorvoloriddle88% (17)
- Ho 1 Forecast Remedial Law PDFDocument53 pagesHo 1 Forecast Remedial Law PDFFrances Ann TevesNo ratings yet
- Leyte Department of Education Personal Development DocumentDocument2 pagesLeyte Department of Education Personal Development DocumentMaricar Cesista NicartNo ratings yet
- Sarah Lowthian.: Hello My Name IsDocument3 pagesSarah Lowthian.: Hello My Name Isapi-225679366No ratings yet
- Understanding Application ReasoningDocument42 pagesUnderstanding Application ReasoningadeNo ratings yet
- Department of History, III BA A' Paper-VI Ancient Karnataka History KNMNC, Shivamogga. Historical SourcesDocument7 pagesDepartment of History, III BA A' Paper-VI Ancient Karnataka History KNMNC, Shivamogga. Historical SourcesBharat KumarNo ratings yet
- Kumpulan Soal SynonymDocument10 pagesKumpulan Soal SynonymMuhammad Abi PrasetyoNo ratings yet
- Partial PulpotomyDocument5 pagesPartial PulpotomyLeena Losheene VijayakumarNo ratings yet
- Petroleum GeologyDocument1 pagePetroleum GeologyRevan AkramNo ratings yet
- Mechatronics Definition:: Task 1 - P1Document7 pagesMechatronics Definition:: Task 1 - P1mrssahar100% (1)