You might also like
- Chiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewDocument23 pagesChiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewEdgardo BivimasNo ratings yet
- Autismand PDDDocument229 pagesAutismand PDDIan BrownNo ratings yet
- Control of Nonconforming Work019 Af.r4Document6 pagesControl of Nonconforming Work019 Af.r4Massimiliano PorcelliNo ratings yet
- Efficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementDocument10 pagesEfficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementChung Tze YangNo ratings yet
- Diagnostic Problems in Tumors of Central Nervous System: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Central Nervous System: Selected TopicsNo ratings yet
- National Rural Health Mission AssignmentDocument12 pagesNational Rural Health Mission AssignmentFaceless BubbiesNo ratings yet
- Jurnal Fraktur PDFDocument9 pagesJurnal Fraktur PDFdwi vaniNo ratings yet
- Medicine: Open Reduction and Plate Fixation Compared With Non-Surgical Treatment For Displaced Midshaft Clavicle FractureDocument16 pagesMedicine: Open Reduction and Plate Fixation Compared With Non-Surgical Treatment For Displaced Midshaft Clavicle Fracturedwi vaniNo ratings yet
- Systematic ReviewDocument7 pagesSystematic ReviewErwin WibowoNo ratings yet
- Midshaft Clavicle Fractures: Surgery Provides Better Results As Compared With Nonoperative TreatmentDocument10 pagesMidshaft Clavicle Fractures: Surgery Provides Better Results As Compared With Nonoperative TreatmentS3V4_9154No ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- 15 Treatment Outcomes of Meniscal Root TearsDocument11 pages15 Treatment Outcomes of Meniscal Root Tearsdados2000No ratings yet
- Best Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Document7 pagesBest Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Tuấn Lê (jose)No ratings yet
- Meniscus Root Repair Vs Meniscectomy orDocument8 pagesMeniscus Root Repair Vs Meniscectomy orJulio Cesar Guillen MoralesNo ratings yet
- 2014 Article 3495Document7 pages2014 Article 3495cogajoNo ratings yet
- Medi 98 E13054Document7 pagesMedi 98 E13054Andrea OsborneNo ratings yet
- Van Midden Dorp 2013Document14 pagesVan Midden Dorp 2013Raveli KalvinNo ratings yet
- Lin 2018Document14 pagesLin 2018giselaNo ratings yet
- Posterior Crossbite and Functional ChangesDocument7 pagesPosterior Crossbite and Functional ChangesFANOR ALFONSO MARTINEZ ARCÓNNo ratings yet
- Review Article: The Role of Fibular Fixation in Distal Tibia-Fibula Fractures: A Meta-AnalysisDocument9 pagesReview Article: The Role of Fibular Fixation in Distal Tibia-Fibula Fractures: A Meta-AnalysisGus AbellaNo ratings yet
- Kovachevich2009 Article OperativeManagementOfTheMedialDocument7 pagesKovachevich2009 Article OperativeManagementOfTheMedialMaddy WolsmenNo ratings yet
- RunningDocument21 pagesRunningHossein NajjarzadeNo ratings yet
- Matsuda 2014Document8 pagesMatsuda 2014Adrian SilaghiNo ratings yet
- 2017 Article 528Document12 pages2017 Article 528Marios GhobrialNo ratings yet
- Stadhouder 2008 SpineDocument12 pagesStadhouder 2008 SpineVijay JephNo ratings yet
- Displaced Distal Radius Fractures in Children, Cast Alone Vs Additional K-Wire Fixation: A Meta-AnalysisDocument9 pagesDisplaced Distal Radius Fractures in Children, Cast Alone Vs Additional K-Wire Fixation: A Meta-AnalysisCharlie CaceresNo ratings yet
- Acl PDFDocument11 pagesAcl PDFDaniela CasabonaNo ratings yet
- MMT Validity ReliabilityDocument23 pagesMMT Validity ReliabilitynNo ratings yet
- Swart 2016Document7 pagesSwart 2016TommysNo ratings yet
- Effectiveness of Micro-Implant in Vertical Control During Orthodontic Treatment of Class II Malocclusion: A Systematic Review and Meta-AnalysisDocument15 pagesEffectiveness of Micro-Implant in Vertical Control During Orthodontic Treatment of Class II Malocclusion: A Systematic Review and Meta-AnalysisThang Nguyen TienNo ratings yet
- Choi 2021Document12 pagesChoi 2021paul_androideNo ratings yet
- The Effectiveness of Rehabilitation For Nonoperative Management of Shoulder Instability - A Systematic ReviewDocument14 pagesThe Effectiveness of Rehabilitation For Nonoperative Management of Shoulder Instability - A Systematic ReviewAlvaro Fabian Córdova WhiteleyNo ratings yet
- Diagnostic Accuracy of Examination Tests For Lateral Elbow Tendinopathy (LET) - A Systematic ReviewDocument10 pagesDiagnostic Accuracy of Examination Tests For Lateral Elbow Tendinopathy (LET) - A Systematic Reviewpatinoomar67No ratings yet
- Jurnal Tendon 1Document10 pagesJurnal Tendon 1hendrabecaxNo ratings yet
- Simple Elbow Dislocation AOTS 2010Document9 pagesSimple Elbow Dislocation AOTS 2010harpreet singhNo ratings yet
- The Influence of Crown-To-Implant Ratio in Single Crowns On Clinical Outcomes - A Systematic Review and Meta-AnalysisDocument6 pagesThe Influence of Crown-To-Implant Ratio in Single Crowns On Clinical Outcomes - A Systematic Review and Meta-Analysiscd.brendasotofloresNo ratings yet
- Clinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisDocument11 pagesClinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisArkar SoeNo ratings yet
- The Treatment of Simple Elbow Dislocation in Adults: Original ArticleDocument9 pagesThe Treatment of Simple Elbow Dislocation in Adults: Original ArticleMukharradhiNo ratings yet
- Gill2021 Article Post-traumaticSplenicInjuryOutDocument10 pagesGill2021 Article Post-traumaticSplenicInjuryOutCarlosA.DíazNo ratings yet
- Patient Outcomes Following Tricompartmental Total Knee Replacement: A Meta-AnalysisDocument3 pagesPatient Outcomes Following Tricompartmental Total Knee Replacement: A Meta-AnalysisSahithya MNo ratings yet
- Review Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-AnalysisDocument15 pagesReview Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-Analysissymbiosis.ikfrNo ratings yet
- Evaluación Clínica y Funcional Del HombroDocument9 pagesEvaluación Clínica y Funcional Del HombroLuis Eduardo Cabezas MirandaNo ratings yet
- Ebp PaperDocument16 pagesEbp Paperapi-583545759No ratings yet
- Accuracy of Clin. Tests 2020Document12 pagesAccuracy of Clin. Tests 2020Ahmed MortadaNo ratings yet
- Artigo LIVE Fukuda (Menisco Hohmann2018)Document10 pagesArtigo LIVE Fukuda (Menisco Hohmann2018)gabynieto.031090No ratings yet
- Rcsann 2016 0048Document6 pagesRcsann 2016 0048fabian arassiNo ratings yet
- J Apergo 2020 103353Document8 pagesJ Apergo 2020 103353helenotatiana24No ratings yet
- 2015 - Article - 665eficacia EpicondilitiDocument13 pages2015 - Article - 665eficacia EpicondilitimorbreirNo ratings yet
- Clavicle ORIFDocument8 pagesClavicle ORIFsefhilla putriNo ratings yet
- Bankart VS Tratamiento ConservadorDocument7 pagesBankart VS Tratamiento ConservadorMaría IsabelNo ratings yet
- Clinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysisDocument8 pagesClinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysissamNo ratings yet
- Hallux MBEDocument12 pagesHallux MBENicolas ReyesNo ratings yet
- Challoumas - 2020 - Oi - 200938 - 1607525668.61599 InglesDocument28 pagesChalloumas - 2020 - Oi - 200938 - 1607525668.61599 Inglesmauricio castroNo ratings yet
- Early Surgery Compared To Nonoperative ManagementDocument11 pagesEarly Surgery Compared To Nonoperative ManagementantoniowidiaNo ratings yet
- 2023 - Surgical Techniques For Medial Patellofemoral LigamentDocument11 pages2023 - Surgical Techniques For Medial Patellofemoral Ligamentorthotraumato30No ratings yet
- #PENTING Demeurechy2018Document19 pages#PENTING Demeurechy2018Octapaedi SoetomoNo ratings yet
- Superior Capsule Reconstruction For Irreparable Massive Rotator Cuff Tears: Does It Make Sense?Document11 pagesSuperior Capsule Reconstruction For Irreparable Massive Rotator Cuff Tears: Does It Make Sense?FelipeSanzanaNo ratings yet
- Zhang2018Document9 pagesZhang2018Rodrigo CarvachoNo ratings yet
- Columna Paper Anato 2Document7 pagesColumna Paper Anato 2Claudio Cofré MansillaNo ratings yet
- Bsms 6Document6 pagesBsms 6Filip starcevicNo ratings yet
- Effects of Rapid Maxillary Expansion On The Midpalatal Suture A Systematic ReviewDocument5 pagesEffects of Rapid Maxillary Expansion On The Midpalatal Suture A Systematic ReviewMariana SantosNo ratings yet
- CBMT and NTDocument11 pagesCBMT and NTrizkiriasariNo ratings yet
- Hook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisDocument6 pagesHook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisFillipe AgraNo ratings yet
- Medi 98 E13054Document7 pagesMedi 98 E13054Andrea OsborneNo ratings yet
- Operative Treatment of Terrible Triad of TheDocument8 pagesOperative Treatment of Terrible Triad of TheAndrea OsborneNo ratings yet
- 1 s2.0 S1877056821003029 MainDocument21 pages1 s2.0 S1877056821003029 MainAndrea OsborneNo ratings yet
- Bulletin of Emergency and TraumaDocument3 pagesBulletin of Emergency and TraumaAndrea OsborneNo ratings yet
- Surgical Treatment For Terrible Triad Injury of The Elbow With Anteromedial Coronoid Fracture Through A Combined Surgical ApproachDocument12 pagesSurgical Treatment For Terrible Triad Injury of The Elbow With Anteromedial Coronoid Fracture Through A Combined Surgical ApproachAndrea OsborneNo ratings yet
- Treatment Strategy of Terrible Triad of The Elbow - Experience in Shanghai 6th People's HospitalDocument7 pagesTreatment Strategy of Terrible Triad of The Elbow - Experience in Shanghai 6th People's HospitalAndrea OsborneNo ratings yet
- Medi 97 E0523Document9 pagesMedi 97 E0523Andrea OsborneNo ratings yet
- 4 Other 17 1 10 20200119Document5 pages4 Other 17 1 10 20200119Andrea OsborneNo ratings yet
- What Factors Are Associated With Elbow Stiffness After Operation of Terrible Triad InjuryDocument16 pagesWhat Factors Are Associated With Elbow Stiffness After Operation of Terrible Triad InjuryAndrea OsborneNo ratings yet
- IJAJR 2018 Long Term Functional Outcomes of The Terrible Triad of The ElbowDocument6 pagesIJAJR 2018 Long Term Functional Outcomes of The Terrible Triad of The ElbowAndrea OsborneNo ratings yet
- Receipt: Aotrauma Seminar-Distal Tibia, Ankle and HindfootDocument1 pageReceipt: Aotrauma Seminar-Distal Tibia, Ankle and HindfootAndrea OsborneNo ratings yet
- Nurshing English 1 S1 Keperawatan Tingkat 2 (40 Prosedur Keperawatan)Document361 pagesNurshing English 1 S1 Keperawatan Tingkat 2 (40 Prosedur Keperawatan)Jankrik BelalangNo ratings yet
- Thapar, Cooper, Eyre y LangleyDocument15 pagesThapar, Cooper, Eyre y LangleyNicol Mariana V. FernándezNo ratings yet
- Nutri QuizDocument70 pagesNutri QuizMary Grace Geronimo SalaysayNo ratings yet
- Predicting The Evolution of Counseling Psychology in TheDocument18 pagesPredicting The Evolution of Counseling Psychology in Thewhether913No ratings yet
- Diagnostic Test-Hg 7Document7 pagesDiagnostic Test-Hg 7Marrie Anne Buena-Agua MercaNo ratings yet
- The Yemen Crisis: Uscri BackgrounderDocument11 pagesThe Yemen Crisis: Uscri BackgrounderJessareth CapacioNo ratings yet
- TESDA Costing 2021 - ADocument2 pagesTESDA Costing 2021 - AAljon BalanagNo ratings yet
- iTT MANUALDocument80 pagesiTT MANUALGerencia Rigar Colombia SASNo ratings yet
- El LHDocument2 pagesEl LHMaherNo ratings yet
- Elbow Rehab UCL Sprain Non OperativeDocument5 pagesElbow Rehab UCL Sprain Non OperativeacfountainNo ratings yet
- 2159-Article Text-4965-1-10-20230310Document7 pages2159-Article Text-4965-1-10-20230310najwaazzahra2121No ratings yet
- Module B - Lesson 5Document17 pagesModule B - Lesson 5Melanie CortezNo ratings yet
- KPPS Dan Linmas PadaasihDocument14 pagesKPPS Dan Linmas PadaasihabdulhalimmuhlisNo ratings yet
- Fourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A SeriesDocument3 pagesFourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A Seriesjoshuaangue60% (5)
- OOS Investigation and Where You Are Going Wrong: Page 1 of 3Document3 pagesOOS Investigation and Where You Are Going Wrong: Page 1 of 3Sangram KendreNo ratings yet
- Goal of IsolationDocument20 pagesGoal of IsolationShivangiJainNo ratings yet
- FIKY NISWATI YUSLIHAH (P17250193025) Part of Body PainDocument6 pagesFIKY NISWATI YUSLIHAH (P17250193025) Part of Body PainFiky NiswatiNo ratings yet
- 6 Middle Facial FracturesDocument29 pages6 Middle Facial FracturesYoussef ElbeharyNo ratings yet
- Thyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Document11 pagesThyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Vaishnavi SheteNo ratings yet
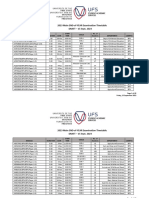
- 2023 Main End of Year Examination Timetable DraftDocument49 pages2023 Main End of Year Examination Timetable DraftmrkoofosuNo ratings yet
- Political SelfDocument53 pagesPolitical SelfMelizza Fajardo BañanoNo ratings yet
- Senior Citizen or Elderly - Any Filipino Citizen Who Is A Resident of The Philippines Who Is 60 Y/o or AboveDocument3 pagesSenior Citizen or Elderly - Any Filipino Citizen Who Is A Resident of The Philippines Who Is 60 Y/o or AboveAlliah SomidoNo ratings yet
- Vytalyze CBD Oil Where To Buy, Read Price, Reviews & Scam!Document3 pagesVytalyze CBD Oil Where To Buy, Read Price, Reviews & Scam!muriellearrNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaEenk RukmanaNo ratings yet
- eكتيب السلامة للمقاولين ISS-03Document40 pageseكتيب السلامة للمقاولين ISS-03SAEED ALGHAMDINo ratings yet
- Hunting Ground SketchDocument2 pagesHunting Ground Sketchapi-3551012790% (1)
- Linking Impression Management As A Precursor For Surface ActingDocument6 pagesLinking Impression Management As A Precursor For Surface ActingInternational Journal of Innovative Science and Research TechnologyNo ratings yet