You might also like
- Peter A. Levine - Waking The Tiger - Healing Trauma - The Innate Capacity To Transform Overwhelming Experiences - 1997 - OCRDocument193 pagesPeter A. Levine - Waking The Tiger - Healing Trauma - The Innate Capacity To Transform Overwhelming Experiences - 1997 - OCRNeelakanta Kalla96% (55)
- Public Value and Art For All?Document20 pagesPublic Value and Art For All?yolandaniguasNo ratings yet
- Sir Syed Ahmed Khan and Two Nation TheoryDocument11 pagesSir Syed Ahmed Khan and Two Nation TheoryZeeshan Saeed100% (5)
- PTV Vissim - First Steps ENG PDFDocument34 pagesPTV Vissim - First Steps ENG PDFBeby RizcovaNo ratings yet
- JNPPR 3 129Document16 pagesJNPPR 3 129Alessandro BergantinNo ratings yet
- Rotator Cuff Related Shoulder Pain Assessment, Management and UncertaintiesDocument37 pagesRotator Cuff Related Shoulder Pain Assessment, Management and UncertaintiesPablo Gómez SotoNo ratings yet
- Clinical Assessment of The Musculoskeletal System: A Guide For Medical Students and Healthcare ProfessionalsDocument40 pagesClinical Assessment of The Musculoskeletal System: A Guide For Medical Students and Healthcare ProfessionalsButchay LumbabNo ratings yet
- Accepted Manuscript: 10.1016/j.jbmt.2017.09.015Document10 pagesAccepted Manuscript: 10.1016/j.jbmt.2017.09.015Daniel GuevaraNo ratings yet
- Peripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeDocument13 pagesPeripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeRafael MoreiraNo ratings yet
- Abstract Leftsidest SetDocument1,047 pagesAbstract Leftsidest Setpokharelriwaj82No ratings yet
- Physical Therapy in Sport: Literature ReviewDocument9 pagesPhysical Therapy in Sport: Literature ReviewPrincess Dianna SulitNo ratings yet
- 1 UsDocument7 pages1 UsJenny VibsNo ratings yet
- J MSKSP 2017 11 003Document16 pagesJ MSKSP 2017 11 003Rui Pedro PereiraNo ratings yet
- Accepted Manuscript: 10.1016/j.clinbiomech.2017.03.004Document30 pagesAccepted Manuscript: 10.1016/j.clinbiomech.2017.03.004Ambar Dani SyuhadaNo ratings yet
- Rehabilitation in MSDocument39 pagesRehabilitation in MSFriendlymeNo ratings yet
- Accepted Manuscript: Journal of Bodywork & Movement TherapiesDocument53 pagesAccepted Manuscript: Journal of Bodywork & Movement TherapiesEduardo Santana SuárezNo ratings yet
- Robotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyDocument9 pagesRobotic Arm-Assisted Versus Manual Total Hip Arthroplasty A Propensity Score Matched Cohort StudyShiv KolheNo ratings yet
- Is Modern Perioperative Care Too Complicated For Surgeons?: ReferencesDocument2 pagesIs Modern Perioperative Care Too Complicated For Surgeons?: ReferencesHasriana BudimanNo ratings yet
- Student Handbook 11-1Document40 pagesStudent Handbook 11-1archmagus2345No ratings yet
- GR Up: SM Orthopedics & Muscular SystemDocument6 pagesGR Up: SM Orthopedics & Muscular SystemValerie BpNo ratings yet
- Franke 2016Document40 pagesFranke 2016M MisbahunnurNo ratings yet
- Evaluación Back Pain Peter o SullivanDocument11 pagesEvaluación Back Pain Peter o SullivanAntonio tapiaNo ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument37 pagesThis Item Is The Archived Peer-Reviewed Author-Version oftri dianaNo ratings yet
- JCM 10 00086 v2Document19 pagesJCM 10 00086 v2Dana DumitruNo ratings yet
- Recording. Churchill Livingstone.: Bibliografie Ortezari Si ProtezariDocument2 pagesRecording. Churchill Livingstone.: Bibliografie Ortezari Si ProtezariOana RuxandraNo ratings yet
- Boom or Bust in OTDocument4 pagesBoom or Bust in OTSusan Ly VillalobosNo ratings yet
- A Systematic Review of Outcomes Reporting For Brachial Plexus ReconstructionDocument6 pagesA Systematic Review of Outcomes Reporting For Brachial Plexus ReconstructionAndrés Urrego NietoNo ratings yet
- Nihms 1606560Document18 pagesNihms 1606560norazmiNo ratings yet
- RATetal IntJClinEpidemio2005Document10 pagesRATetal IntJClinEpidemio2005BRAIN SHARPNERNo ratings yet
- Journal of Yoga and Physical TherapyDocument1 pageJournal of Yoga and Physical Therapykhadesakshi55No ratings yet
- Effects of Adding A Neurodynamic Mobilization To Motor Control Training in Patients With Lumbar Radiculopathy Due To DiscDocument33 pagesEffects of Adding A Neurodynamic Mobilization To Motor Control Training in Patients With Lumbar Radiculopathy Due To Discmarcelogascon.oNo ratings yet
- Ijerph 18 01630Document13 pagesIjerph 18 01630ع الNo ratings yet
- Educating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SDocument10 pagesEducating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SjotaNo ratings yet
- I C M M, M O, H P A M T P - F H P: A R C TDocument9 pagesI C M M, M O, H P A M T P - F H P: A R C TAngie D. AndradesNo ratings yet
- Bab 2Document2 pagesBab 2SANDA NABILAH FATINNo ratings yet
- Cheung2020 PDFDocument15 pagesCheung2020 PDFSandra Milena Cortes SotoNo ratings yet
- Surgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsDocument8 pagesSurgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsLuis Carlos HernandezNo ratings yet
- Within Day and Between Day RelDocument22 pagesWithin Day and Between Day RelgtzjeNo ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- 10 1016@j Ultrasmedbio 2020 02 004Document15 pages10 1016@j Ultrasmedbio 2020 02 004Humberto Salas VelizNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Manual Therapy: Filip Struyf, Jo Nijs, Stijn Horsten, Sarah Mottram, Steven Truijen, Romain MeeusenDocument6 pagesManual Therapy: Filip Struyf, Jo Nijs, Stijn Horsten, Sarah Mottram, Steven Truijen, Romain MeeusenJorgeNo ratings yet
- Jacobson 2012Document8 pagesJacobson 2012Waqas HaleemNo ratings yet
- BMR - 2022 - 35 3 - BMR 35 3 bmr210053 - BMR 35 bmr210053Document15 pagesBMR - 2022 - 35 3 - BMR 35 3 bmr210053 - BMR 35 bmr210053Nicol Sandoval SotoNo ratings yet
- Chronic Daily Headache: Suggestion For The Neuromuscular Oral TherapyDocument4 pagesChronic Daily Headache: Suggestion For The Neuromuscular Oral TherapyFuioaga Codrin-PaulNo ratings yet
- Critical Window For Recovery in StrokeDocument8 pagesCritical Window For Recovery in StrokeJerrin JacobNo ratings yet
- Rehabilitation HipDocument29 pagesRehabilitation HipZahraa MNo ratings yet
- 2012 If Exercise Is Medicine, Who Should Be The PrescriberDocument2 pages2012 If Exercise Is Medicine, Who Should Be The PrescriberCristiano MatosNo ratings yet
- The Role of Biofeedback in Stroke Rehabilitation: Past and Future DirectionsDocument9 pagesThe Role of Biofeedback in Stroke Rehabilitation: Past and Future Directionsnandhini raguNo ratings yet
- To Medical PhysicsDocument165 pagesTo Medical PhysicsHUAWEI HUAWEINo ratings yet
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanNo ratings yet
- Research Study DesignsDocument2 pagesResearch Study DesignsAshley WuNo ratings yet
- Pi Is 0161475415000706Document14 pagesPi Is 0161475415000706Zumrotul MinaNo ratings yet
- Clinical Practice and Effectiveness of Kinesio Taping For Lower Limb Musculoskeletal Disorder: A Systematic AppraisalDocument15 pagesClinical Practice and Effectiveness of Kinesio Taping For Lower Limb Musculoskeletal Disorder: A Systematic Appraisalد.موسى التويتيNo ratings yet
- 10 1016@j Math 2013 12 002Document21 pages10 1016@j Math 2013 12 002BetoNo ratings yet
- Enoka 2015Document42 pagesEnoka 2015javiNo ratings yet
- Ankle Sprain CPR For ManipulationDocument13 pagesAnkle Sprain CPR For ManipulationChaim MalineNo ratings yet
- Unal 2016Document21 pagesUnal 2016Deni MalikNo ratings yet
- Osteoarthritis Year in Review: Outcome of Rehabilitation: Yzx Yk (Document11 pagesOsteoarthritis Year in Review: Outcome of Rehabilitation: Yzx Yk (Nurfitrianti ArfahNo ratings yet
- Management of Cerebral Palsy: A Literature Review From A Physiatric PerspectiveDocument4 pagesManagement of Cerebral Palsy: A Literature Review From A Physiatric Perspectivefebry firmansyahNo ratings yet
- Clinical ResearcheffectsDocument7 pagesClinical ResearcheffectsJackielyn C. AportaderaNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- Treadmill Training and Kinesiotherapy Versus Conventional Physiotherapy in Parkinson's Disease: A Pragmatic StudyDocument8 pagesTreadmill Training and Kinesiotherapy Versus Conventional Physiotherapy in Parkinson's Disease: A Pragmatic StudylscmaristelaNo ratings yet
- PGCC 2022 HandbookDocument17 pagesPGCC 2022 HandbookhasnainNo ratings yet
- Eyu-Ethiopia FinanceOperations Manual January2020 v1 EnglishDocument104 pagesEyu-Ethiopia FinanceOperations Manual January2020 v1 EnglishHenockNo ratings yet
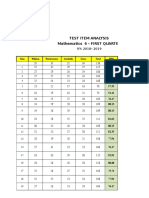
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet
- Rod and Pump DataDocument11 pagesRod and Pump DataYoandri Stefania Guerrero CamargoNo ratings yet
- CHED - NYC PresentationDocument19 pagesCHED - NYC PresentationMayjee De La CruzNo ratings yet
- Project PlanDocument3 pagesProject PlanEarl Dave NangganNo ratings yet
- HW 2Document12 pagesHW 2Munish RanaNo ratings yet
- PointgroupsDocument13 pagesPointgroupsT alameluNo ratings yet
- The Enemy Within - v18Document8 pagesThe Enemy Within - v18Matt WillisNo ratings yet
- Logix 5000 Controllers Tasks, Programs, and RoutinesDocument73 pagesLogix 5000 Controllers Tasks, Programs, and Routinesobi SalamNo ratings yet
- Phys172 S20 Lab07 FinalDocument8 pagesPhys172 S20 Lab07 FinalZhuowen YaoNo ratings yet
- Chapter 3 QuantiDocument5 pagesChapter 3 QuantiChristine NavidadNo ratings yet
- Module 2 Tssig Week 2 3Document4 pagesModule 2 Tssig Week 2 3Alysa QuintanarNo ratings yet
- Vasuanand Bba ProjectDocument66 pagesVasuanand Bba ProjectMaster PrintersNo ratings yet
- Civil Engineering MCQ'sDocument1 pageCivil Engineering MCQ'sNISHIKANTA MONDALNo ratings yet
- Passenger Elevator Operation ManualDocument24 pagesPassenger Elevator Operation ManualJahn Ray B. Lanozo100% (1)
- Rasi Navamsa: As Mo Ke Su Ve Mo JuDocument11 pagesRasi Navamsa: As Mo Ke Su Ve Mo JuRavan SharmaNo ratings yet
- Sky & Telescope - February 2016 (Gnv64)Document82 pagesSky & Telescope - February 2016 (Gnv64)bogarguz100% (1)
- I Can Learn English 1Document100 pagesI Can Learn English 1IbetNo ratings yet
- 22445-2022-Summer-Model-Answer-Paper (Msbte Study Resources)Document27 pages22445-2022-Summer-Model-Answer-Paper (Msbte Study Resources)Piyush NikamNo ratings yet
- Conscious Sedation PaediatricsDocument44 pagesConscious Sedation PaediatricsReeta TaxakNo ratings yet
- British Food Journal: Article InformationDocument8 pagesBritish Food Journal: Article InformationanisaNo ratings yet
- HW1Document5 pagesHW1John SpartanNo ratings yet
- Question BankDocument9 pagesQuestion Bankpragash100% (1)
- Penjelasan IMRAD StructureDocument2 pagesPenjelasan IMRAD Structureaji bondesNo ratings yet
- Grammar Translation MethodDocument22 pagesGrammar Translation MethodCeyinNo ratings yet