You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Management by ObjectivesDocument30 pagesManagement by ObjectivesJasmandeep brar100% (4)
- Hortors Online ManualDocument11 pagesHortors Online Manualtshepang4228No ratings yet
- Bar Q Salaries Part 2Document5 pagesBar Q Salaries Part 2Brigette DomingoNo ratings yet
- Lesson For SpreadsheetsDocument69 pagesLesson For SpreadsheetsCrisna Rivera PundanoNo ratings yet
- Media and Information Literacy Quarter 3 Module 1Document67 pagesMedia and Information Literacy Quarter 3 Module 1Joshua Catequesta100% (1)
- HANA Heroes 1 - EWM Lessons Learned (V2)Document40 pagesHANA Heroes 1 - EWM Lessons Learned (V2)Larissa MaiaNo ratings yet
- Questions & Answers On CountersDocument24 pagesQuestions & Answers On Counterskibrom atsbha100% (2)
- JKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralDocument270 pagesJKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralYamie Rozman100% (1)
- Google-Analytics 01Document28 pagesGoogle-Analytics 01Smm Store24No ratings yet
- Morales v. Lockheed Martin, 10th Cir. (2000)Document2 pagesMorales v. Lockheed Martin, 10th Cir. (2000)Scribd Government DocsNo ratings yet
- Oxford Handbooks Online: From Old To New Developmentalism in Latin AmericaDocument27 pagesOxford Handbooks Online: From Old To New Developmentalism in Latin AmericadiegoNo ratings yet
- Business Works Student User GuideDocument14 pagesBusiness Works Student User GuideAkram UddinNo ratings yet
- On Fracture MechanicsDocument81 pagesOn Fracture MechanicsDEEPAK100% (1)
- Tesco Travel Policy BookletDocument64 pagesTesco Travel Policy Bookletuser001hNo ratings yet
- Soal TKM B. Inggris Kls XII Des. 2013Document8 pagesSoal TKM B. Inggris Kls XII Des. 2013Sinta SilviaNo ratings yet
- Choosing The Right HF Welding Process For Api Large Pipe MillsDocument5 pagesChoosing The Right HF Welding Process For Api Large Pipe MillsNia KurniaNo ratings yet
- 3d Mug Tutorial in 3d MaxDocument5 pages3d Mug Tutorial in 3d MaxCalvin TejaNo ratings yet
- Hyster Forklift Class 5 Internal Combustion Engine Trucks g019 h13xm h12xm 12ec Service ManualsDocument23 pagesHyster Forklift Class 5 Internal Combustion Engine Trucks g019 h13xm h12xm 12ec Service Manualsedwinodom070882sad100% (72)
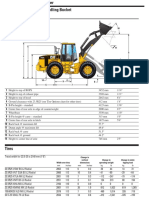
- Cat It62hDocument4 pagesCat It62hMarceloNo ratings yet
- LESSON - STEM-based Research ProblemsDocument49 pagesLESSON - STEM-based Research ProblemsLee JenoNo ratings yet
- Accomplishment Report Dictrict Preventive MaintenanceDocument2 pagesAccomplishment Report Dictrict Preventive MaintenanceZenia CapalacNo ratings yet
- 2B. Glicerina - USP-NF-FCC Glycerin Nutritional Statement USP GlycerinDocument1 page2B. Glicerina - USP-NF-FCC Glycerin Nutritional Statement USP Glycerinchristian muñozNo ratings yet
- Sec 11Document3 pagesSec 11Vivek JhaNo ratings yet
- Pub 005940 PDFDocument31 pagesPub 005940 PDFkurniaNo ratings yet
- Partes Oki - MPS5501B - RSPL - Rev - HDocument12 pagesPartes Oki - MPS5501B - RSPL - Rev - HJaiber Eduardo Gutierrez OrtizNo ratings yet
- Hydraulic Breakers in Mining ApplicationDocument28 pagesHydraulic Breakers in Mining ApplicationdrmassterNo ratings yet
- County Project Name Cycle Project Address Proj City Proj Zip Applicant/Owner Name HDGP $ Home $ FHTF $ Lihtc9 $ Help $ Oahtc $ Ghap $ HPF $ Lihtc4 $Document60 pagesCounty Project Name Cycle Project Address Proj City Proj Zip Applicant/Owner Name HDGP $ Home $ FHTF $ Lihtc9 $ Help $ Oahtc $ Ghap $ HPF $ Lihtc4 $Mamello PortiaNo ratings yet
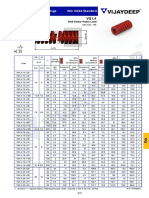
- Rectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadDocument3 pagesRectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadbashaNo ratings yet
- IM0973567 Orlaco EMOS Photonview Configuration EN A01 MailDocument14 pagesIM0973567 Orlaco EMOS Photonview Configuration EN A01 Maildumass27No ratings yet
- Human Resource Management - Introduction - A Revision Article - A Knol by Narayana RaoDocument7 pagesHuman Resource Management - Introduction - A Revision Article - A Knol by Narayana RaoHimanshu ShuklaNo ratings yet