You might also like
- Optic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraDocument21 pagesOptic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraAqsaNo ratings yet
- Pupillary Dilatation ReflexDocument7 pagesPupillary Dilatation ReflexEden Canonizado ChengNo ratings yet
- Cranial Nerve Nadz FinalDocument58 pagesCranial Nerve Nadz Finalnadzirah ruslanNo ratings yet
- The Swinging Flashlight Test: Learning Objective: Facts About The PupilDocument3 pagesThe Swinging Flashlight Test: Learning Objective: Facts About The Pupilsiti hazard aldinaNo ratings yet
- StrokeDocument27 pagesStrokeSameen ArshadNo ratings yet
- Traumatic Brain Injury: Shantaveer Gangu Mentor-Dr - Baldauf MDDocument53 pagesTraumatic Brain Injury: Shantaveer Gangu Mentor-Dr - Baldauf MDRio AlexanderNo ratings yet
- Mood Disorders After TBIDocument17 pagesMood Disorders After TBIJaun CarrilloNo ratings yet
- Stroke: Pathophysiology, Types, Management Categories, and Vascular SyndromesDocument49 pagesStroke: Pathophysiology, Types, Management Categories, and Vascular Syndromesrabia khalidNo ratings yet
- Head and Spinal Cord Injury (Ci)Document111 pagesHead and Spinal Cord Injury (Ci)azmerawNo ratings yet
- AdelineDocument34 pagesAdelineEmmanuel NdukaNo ratings yet
- A Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosisDocument7 pagesA Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosistiaraleshaNo ratings yet
- Cerebrovascular Diseases Risk Factors:: o o o o oDocument4 pagesCerebrovascular Diseases Risk Factors:: o o o o otrinaNo ratings yet
- Traumatic Brain Injury 1Document33 pagesTraumatic Brain Injury 1Bright SunshinenNo ratings yet
- Head Trauma PDFDocument16 pagesHead Trauma PDFCharlene FernándezNo ratings yet
- 2015 Vascular DementiaDocument9 pages2015 Vascular DementiajavierNo ratings yet
- Traumatic Brain InjuryDocument40 pagesTraumatic Brain InjuryRed DevilNo ratings yet
- Head TraumaDocument15 pagesHead TraumaDede Yusuf FNo ratings yet
- Neuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawangDocument65 pagesNeuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawanggeorgyNo ratings yet
- Neurology Topics: Degenerative DiseasesDocument57 pagesNeurology Topics: Degenerative Diseasesलुकास विडालNo ratings yet
- OphthalmologyDocument98 pagesOphthalmologyMahmud DipuNo ratings yet
- Intensive Care Nursery: House Staff ManualDocument187 pagesIntensive Care Nursery: House Staff ManualAna MariaNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjuryBelle CaharopNo ratings yet
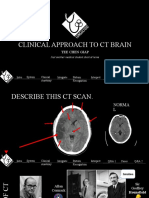
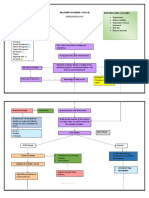
- Clinical Approach To CT BrainDocument34 pagesClinical Approach To CT BrainXiaoThoong LohNo ratings yet
- Visual Field Defect Case ReportDocument25 pagesVisual Field Defect Case Report033010969No ratings yet
- M A N A G E M E NT OF H E A D I NJ UR Y & I NT R A CR A N I A L P RE SS UR EDocument19 pagesM A N A G E M E NT OF H E A D I NJ UR Y & I NT R A CR A N I A L P RE SS UR EmugihartadiNo ratings yet
- Therapeutics of Alzheimer's DiseaseDocument24 pagesTherapeutics of Alzheimer's DiseaseArtemis LiNo ratings yet
- DD Nyeri Kepala Skenario 1Document8 pagesDD Nyeri Kepala Skenario 1Ika Putri YulianiNo ratings yet
- College of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisDocument9 pagesCollege of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisAmlan jyoti thanapati100% (1)
- Prognosis For Healthcare: The Future of Medicine: Bruce M. Cohen, M.D., PH.DDocument46 pagesPrognosis For Healthcare: The Future of Medicine: Bruce M. Cohen, M.D., PH.DSandeshGiriNo ratings yet
- TF00001028 (Autosaved)Document10 pagesTF00001028 (Autosaved)Cid MusaNo ratings yet
- Neurology: Timothy E. Welty, Pharm.D., FCCP, BCPSDocument68 pagesNeurology: Timothy E. Welty, Pharm.D., FCCP, BCPSAlmaha AlfakhriNo ratings yet
- Childhood Epilepsy Etiology, Epidemiology & ManagementDocument6 pagesChildhood Epilepsy Etiology, Epidemiology & ManagementJosh RoshalNo ratings yet
- 2002, Vol.86, Issues 3, DementiaDocument219 pages2002, Vol.86, Issues 3, DementiaCesar GentilleNo ratings yet
- Blood Pressure and The Brain The Neurology of Hypertension PDFDocument12 pagesBlood Pressure and The Brain The Neurology of Hypertension PDFGustavo PestanaNo ratings yet
- Head InjuryDocument31 pagesHead InjuryBoby SuryawanNo ratings yet
- Nystagmus and Localizing ValuesDocument9 pagesNystagmus and Localizing Valueshikmat sheraniNo ratings yet
- Head Injury With Craniotomy A Case Presentation of BSN 3 YB 7Document90 pagesHead Injury With Craniotomy A Case Presentation of BSN 3 YB 7MARIA STEPHANY DELA CRUZNo ratings yet
- Parkinson Disease Pharmacotherapy GuideDocument91 pagesParkinson Disease Pharmacotherapy GuideHsn Tuyết HàNo ratings yet
- Cerebrovascular Disorders: Causes, Types, Symptoms & Treatment of StrokesDocument4 pagesCerebrovascular Disorders: Causes, Types, Symptoms & Treatment of StrokesMhae De GuzmanNo ratings yet
- Etiology and Classification of StrokeDocument10 pagesEtiology and Classification of Strokeaeiou33No ratings yet
- Carotid Artery Dissection PDFDocument3 pagesCarotid Artery Dissection PDFOdranoelRichamNo ratings yet
- Meningitis Pada AnakDocument14 pagesMeningitis Pada AnakRayhanun MardhatillahNo ratings yet
- Transient Ischemic Attack Precipitating Factors Predisposing FactorsDocument6 pagesTransient Ischemic Attack Precipitating Factors Predisposing FactorsYosef OxinioNo ratings yet
- Case Presentation 1Document70 pagesCase Presentation 1shadow gonzalezNo ratings yet
- Red Eye: A Guide For Non-Specialists: MedicineDocument14 pagesRed Eye: A Guide For Non-Specialists: MedicineFapuw Parawansa100% (1)
- PRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewDocument5 pagesPRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewAvicena M IqbalNo ratings yet
- Review To CNS Radiology Including SSDocument52 pagesReview To CNS Radiology Including SSBisher Al-halabiNo ratings yet
- Understanding Stroke and HemiplegiaDocument17 pagesUnderstanding Stroke and HemiplegiaSathias SundariNo ratings yet
- The Second Edition Expert Consensus Statements On The Use of IVIg in NeurologyDocument134 pagesThe Second Edition Expert Consensus Statements On The Use of IVIg in NeurologyRonald DewaNo ratings yet
- MD Papers NewDocument27 pagesMD Papers NewVinay V KulkarniNo ratings yet
- Neurocircuitry of AddictionFrom EverandNeurocircuitry of AddictionNicholas W. GilpinNo ratings yet
- Secondary Fracture Prevention: An International PerspectiveFrom EverandSecondary Fracture Prevention: An International PerspectiveMarkus J. SeibelNo ratings yet
- Soal Ujian NeurotraumaDocument22 pagesSoal Ujian NeurotraumaTina HerreraNo ratings yet
- NCP MeningitisDocument4 pagesNCP MeningitisMa. Gina DerlaNo ratings yet
- Finished Head Injury Ppt-1Document76 pagesFinished Head Injury Ppt-1Chalie MequanentNo ratings yet
- Brain Injury Diagnosis and Treatment After Head TraumaDocument18 pagesBrain Injury Diagnosis and Treatment After Head TraumaMarcela SolarteNo ratings yet
- Visual Field DefectsDocument1 pageVisual Field DefectsLauren LevyNo ratings yet
- 1 My Trigeminal NerveDocument23 pages1 My Trigeminal NerveDan 04No ratings yet
- Subarachnoid Hemorrhage in The Emergency DepartmentDocument8 pagesSubarachnoid Hemorrhage in The Emergency DepartmentLuis octavio carranzaNo ratings yet
- B5W1L9.Peripheral Neuropathy - Lecture Notes 12Document4 pagesB5W1L9.Peripheral Neuropathy - Lecture Notes 12mihalcea alinNo ratings yet
- Brain Death DiagnosisDocument86 pagesBrain Death Diagnosisharsha mummaka100% (1)
- Palliative Care in AdvancedDocument24 pagesPalliative Care in AdvancedClaudio Silva FilhoNo ratings yet
- Reinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFDocument535 pagesReinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFMuhammad HabiburrahmanNo ratings yet
- 01-Guidelines For Use of Hypertonic SalineDocument13 pages01-Guidelines For Use of Hypertonic SalineSatish VeerlaNo ratings yet
- Neuro Exam - Clinical NeurologyDocument38 pagesNeuro Exam - Clinical NeurologyIustitia Septuaginta SambenNo ratings yet
- STROKEDocument9 pagesSTROKEhillary elsaNo ratings yet
- Head Trauma: Yoon Seung-Hwan, M.DDocument53 pagesHead Trauma: Yoon Seung-Hwan, M.DAhmed ZahranNo ratings yet
- TBI QuizletDocument4 pagesTBI QuizletLoraine CometaNo ratings yet
- Cerebral Edema Management ReviewDocument6 pagesCerebral Edema Management ReviewSuryadi P. Dwipayana, Ida BgsNo ratings yet
- Shock TraumaDocument37 pagesShock TraumaMaica LectanaNo ratings yet
- Intracranial Pressure (ICP) : Causes, Concerns and ManagementDocument37 pagesIntracranial Pressure (ICP) : Causes, Concerns and ManagementGus LionsNo ratings yet
- Imaging Tutorial - Differential Diagnosis of Bright Lesions On Diffusion-Weighted MR Images - RadioGraphicsDocument163 pagesImaging Tutorial - Differential Diagnosis of Bright Lesions On Diffusion-Weighted MR Images - RadioGraphicsNatalia E PenagosNo ratings yet
- Brain Trauma Edeme HGDocument15 pagesBrain Trauma Edeme HGiulia lupascuNo ratings yet
- GENERAL LINE of Treatment UREA AMMONIA SALT - poISONINGDocument49 pagesGENERAL LINE of Treatment UREA AMMONIA SALT - poISONINGSunil0% (1)
- Pub - Principles and Practice of NeuropathologyDocument608 pagesPub - Principles and Practice of NeuropathologyArkham AsylumNo ratings yet
- Craniotomy for Subdural HemorrhageDocument28 pagesCraniotomy for Subdural HemorrhageDeinielle Magdangal RomeroNo ratings yet
- Neuromonitoring in Critically Ill Patients.9Document18 pagesNeuromonitoring in Critically Ill Patients.9Israel Villalba FonsecaNo ratings yet
- Traduccion Neurointensivismo Fluidoterapia en Paciente NeurocriticoDocument12 pagesTraduccion Neurointensivismo Fluidoterapia en Paciente NeurocriticoAlanNo ratings yet
- Me Pediatrics Ntruhs Previous Question Papers Chapter WiseDocument9 pagesMe Pediatrics Ntruhs Previous Question Papers Chapter WiseNarendra AnnaladasuNo ratings yet
- Approach to Comatose PatientDocument7 pagesApproach to Comatose PatientROBINSON AYALA GARCIANo ratings yet
- ICP Management Guideline Adult January 2017Document20 pagesICP Management Guideline Adult January 2017syhsyhsyh123No ratings yet
- Johns Hopkins DKA Clinical PathwayDocument31 pagesJohns Hopkins DKA Clinical PathwayPatricia Denise Tome MagisaNo ratings yet
- Neuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaDocument59 pagesNeuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaNovasiska Indriyani HutajuluNo ratings yet
- Intracranial Aneurysms and SAH: Philippe Younes MD Neurosurgeon Head of Neuroscience Department BMCDocument37 pagesIntracranial Aneurysms and SAH: Philippe Younes MD Neurosurgeon Head of Neuroscience Department BMCHussein TarhiniNo ratings yet
- Head TraumaDocument10 pagesHead TraumaVlad ZecaNo ratings yet
- CCU NCP Week 2Document4 pagesCCU NCP Week 2April Kate BanagodosNo ratings yet
- Step LadderExpansive Cranioplasty Mathametical ModelDocument7 pagesStep LadderExpansive Cranioplasty Mathametical ModelDebashree SenguptaNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- Clinical Efficacy of Mannitol (10%) With Glycerine (10%) Versus Mannitol (20%) in Cerebral OedemaDocument6 pagesClinical Efficacy of Mannitol (10%) With Glycerine (10%) Versus Mannitol (20%) in Cerebral OedemaLailNo ratings yet
- 2021 HiponatremiaDocument9 pages2021 HiponatremianaanrvNo ratings yet