You might also like
- Basic Life Support (BLS) Provider HandbookFrom EverandBasic Life Support (BLS) Provider HandbookRating: 5 out of 5 stars5/5 (2)
- Med Surge 2 Mod 3 Study Guide2Document21 pagesMed Surge 2 Mod 3 Study Guide2Dirk Buckner100% (4)
- 7a Summary SheetDocument2 pages7a Summary SheetNoor Ulain NabeelaNo ratings yet
- Assessment of The Acutely Ill PatientDocument10 pagesAssessment of The Acutely Ill PatientZacmilo Dela TorreNo ratings yet
- Assessment of An ICU PatientDocument71 pagesAssessment of An ICU PatientTito Tesfaye100% (1)
- Trauma and Shock ATLSDocument19 pagesTrauma and Shock ATLSDrChauhan100% (2)
- Core ACLS ConceptsDocument60 pagesCore ACLS ConceptsLex CatNo ratings yet
- ABCDE Approach to Assessing and Treating the Acutely Ill PatientDocument22 pagesABCDE Approach to Assessing and Treating the Acutely Ill PatientSarah RamliNo ratings yet
- Anatomy and Physiology of The HeartDocument9 pagesAnatomy and Physiology of The HeartNina Anne ParacadNo ratings yet
- How To Develop Programs For SAP Mobile RFDocument21 pagesHow To Develop Programs For SAP Mobile RFSammy SeidenNo ratings yet
- Triphasic Training Aerobic Block GoalsDocument26 pagesTriphasic Training Aerobic Block GoalsSergi ManzanoNo ratings yet
- Chapter 35 Plant Structure Growth and DevelopmentDocument3 pagesChapter 35 Plant Structure Growth and DevelopmentmokeymonkeyNo ratings yet
- 2020 AHA Guidelines For CPR & ECCDocument42 pages2020 AHA Guidelines For CPR & ECCArun100% (1)
- Oxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CareDocument55 pagesOxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CaretorreslysNo ratings yet
- 004 Practical-Manual PDFDocument72 pages004 Practical-Manual PDFRicardo Domingos100% (1)
- Hypovolemic Shock Nursing Care Management and Study GuideDocument1 pageHypovolemic Shock Nursing Care Management and Study GuideRoselyn VelascoNo ratings yet
- NCP - Ineffective Airway ClearanceDocument2 pagesNCP - Ineffective Airway Clearancelarapatricia1215No ratings yet
- HESI Hints + More Chapter 1-Intro To TestingDocument29 pagesHESI Hints + More Chapter 1-Intro To TestingAngel Nwankwo100% (2)
- MODULE-4 MidtermDocument11 pagesMODULE-4 MidtermQwerty UuNo ratings yet
- Emergency Drugs (LEAD)Document8 pagesEmergency Drugs (LEAD)RayePrudenteNo ratings yet
- DX Intracranial Pressure PDFDocument8 pagesDX Intracranial Pressure PDFSherree HayesNo ratings yet
- Secret Tan Tien rotation technique of Chen Tai ChiDocument4 pagesSecret Tan Tien rotation technique of Chen Tai ChiAmr ElDisouky100% (1)
- Causes and Management of Syncope in DentistryDocument27 pagesCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Chapter 8A Neonatal Emergencies.Document35 pagesChapter 8A Neonatal Emergencies.Sai NathNo ratings yet
- Introduction to Critical illness (3)Document32 pagesIntroduction to Critical illness (3)favourednancie9No ratings yet
- Hypovolemic Shock Neurogenic ShockDocument40 pagesHypovolemic Shock Neurogenic ShockWemslaiNo ratings yet
- Case Study 1 - Head InjuryDocument9 pagesCase Study 1 - Head InjuryTara McNeillNo ratings yet
- Shock PresentationDocument20 pagesShock Presentationrosalyn sugayNo ratings yet
- Hypovolemic and Anaphylactic ShockDocument38 pagesHypovolemic and Anaphylactic ShockJennifer AmbrosioNo ratings yet
- ASSIGNMENT ON SHOCK (SEPTIC SHOCK) (AutoRecovered) (AutoRecovered)Document17 pagesASSIGNMENT ON SHOCK (SEPTIC SHOCK) (AutoRecovered) (AutoRecovered)SabariNo ratings yet
- Pead TraumaDocument33 pagesPead Traumaapi-27208405No ratings yet
- Seminar On Shock c2Document65 pagesSeminar On Shock c2mubarak abdulkadirNo ratings yet
- S. 14.0 Fluid Therapy - Trauma CasesDocument7 pagesS. 14.0 Fluid Therapy - Trauma CasesroropujiNo ratings yet
- Ijccm 23 129Document8 pagesIjccm 23 129Jean Brando Torres GuerreroNo ratings yet
- Emergency MedDocument2 pagesEmergency MedSimp licityNo ratings yet
- Comprehensive Emergency Care ApproachDocument6 pagesComprehensive Emergency Care ApproachBerliana ZaghiNo ratings yet
- Cardiac Life Support Manual-Thiru 2016 -Revised (Repaired)_Aug 2017Document92 pagesCardiac Life Support Manual-Thiru 2016 -Revised (Repaired)_Aug 2017Petracharles AkashiNo ratings yet
- Pediatric Shock: A Guide to Identification, Classification and Initial ManagementDocument20 pagesPediatric Shock: A Guide to Identification, Classification and Initial ManagementvgmanjunathNo ratings yet
- Mechanism of TraumaDocument46 pagesMechanism of TraumauutNo ratings yet
- Severe Sepsisand Septic Shock GuidelinesDocument17 pagesSevere Sepsisand Septic Shock GuidelinesdrquamrulNo ratings yet
- Septic Shock in Children - Rapid Recognition and Initial Resuscitation (First Hour) PDFDocument18 pagesSeptic Shock in Children - Rapid Recognition and Initial Resuscitation (First Hour) PDFLilik NatasubrataNo ratings yet
- Rjpo - JF - Maret 2011Document62 pagesRjpo - JF - Maret 2011Mell-JasmineNo ratings yet
- CHQ GDL 60010 SepsisDocument11 pagesCHQ GDL 60010 SepsissolidtapeNo ratings yet
- Management of Shock in ChildrenDocument26 pagesManagement of Shock in ChildrenkarinakerenNo ratings yet
- paediatric-septic-shockDocument34 pagespaediatric-septic-shockSudha YadavNo ratings yet
- DAY 6 SHOCK StudentsDocument38 pagesDAY 6 SHOCK StudentsTrisha UmaliNo ratings yet
- Guidelines For The Management of Cardiovascular Diseases in IndiaDocument39 pagesGuidelines For The Management of Cardiovascular Diseases in IndiaIndra FauziNo ratings yet
- Ns. AGUS HARYANTO, S Kep Webinar SepsisDocument22 pagesNs. AGUS HARYANTO, S Kep Webinar SepsisDebby F. HandayaniNo ratings yet
- SurgDocument8 pagesSurgJudi Townsend100% (1)
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- ICP and TIADocument4 pagesICP and TIANurse AmbassadorsNo ratings yet
- Emergencies in Dental Clinic: How To DealDocument94 pagesEmergencies in Dental Clinic: How To DealhassonamonaNo ratings yet
- Initial Management of Shock in ChildrenDocument20 pagesInitial Management of Shock in ChildrenPastor Aguirre LópezNo ratings yet
- English Lingo SurgicalDocument36 pagesEnglish Lingo SurgicalObydaNo ratings yet
- MKSAP Questions: Intern ReportDocument37 pagesMKSAP Questions: Intern Reportfidelurtecho4881No ratings yet
- Shock 19Document7 pagesShock 19Teema UmarNo ratings yet
- Clinical Pathway Peds Sepsis 2012Document3 pagesClinical Pathway Peds Sepsis 2012Kim MedairosNo ratings yet
- 099 B SaroshDocument14 pages099 B SaroshUmair AnsariNo ratings yet
- Dentistry L5 SHOCKDocument20 pagesDentistry L5 SHOCKHadeer WasfyNo ratings yet
- Anaphylaxis Acute Management ABCDEDocument8 pagesAnaphylaxis Acute Management ABCDESSNo ratings yet
- Nursing Care Plan For Acute Head InjuryDocument4 pagesNursing Care Plan For Acute Head InjuryAngie Mandeoya67% (3)
- CSS - Advanced Life SupportDocument16 pagesCSS - Advanced Life SupportnrahmaNo ratings yet
- Increased ICPDocument22 pagesIncreased ICPCHARLOTTE DU PREEZNo ratings yet
- Ischemic Stroke ManagementDocument8 pagesIschemic Stroke ManagementBa LitNo ratings yet
- Stabilisasi Resp & HemidinamikDocument30 pagesStabilisasi Resp & HemidinamikBetrice KotanNo ratings yet
- Pediatric Septik ShockDocument37 pagesPediatric Septik Shockmuhammad ismailNo ratings yet
- RF Programming GuideDocument35 pagesRF Programming GuideLaxmikant RathiNo ratings yet
- Bapi Doc PostDocument3 pagesBapi Doc PostLaxmikant RathiNo ratings yet
- Ameya Precision IPO detailsDocument283 pagesAmeya Precision IPO detailsLaxmikant RathiNo ratings yet
- Horizontal SapDocument1 pageHorizontal SapLaxmikant RathiNo ratings yet
- Nirjala EkadasiDocument3 pagesNirjala EkadasiLaxmikant RathiNo ratings yet
- Coins - Know MoreDocument1 pageCoins - Know MoreLaxmikant RathiNo ratings yet
- Payment ReceiptDocument1 pagePayment ReceiptLaxmikant RathiNo ratings yet
- Test Basic IDocument1 pageTest Basic ILaxmikant RathiNo ratings yet
- 2.maks Energy Solutions - GIDDocument40 pages2.maks Energy Solutions - GIDLaxmikant RathiNo ratings yet
- Correspondence Systems TestDocument1 pageCorrespondence Systems TestLaxmikant RathiNo ratings yet
- Notice of 26th Annual General MeetingDocument12 pagesNotice of 26th Annual General MeetingLaxmikant RathiNo ratings yet
- Handling Multi-Byte CharactersDocument2 pagesHandling Multi-Byte CharactersLaxmikant RathiNo ratings yet
- Form Top of Page For Multiple Subheadings in One RowDocument4 pagesForm Top of Page For Multiple Subheadings in One RowLaxmikant RathiNo ratings yet
- Report ZSPOOLTOPDF EmailDocument7 pagesReport ZSPOOLTOPDF EmailLaxmikant RathiNo ratings yet
- ALV - Word WrapDocument4 pagesALV - Word WrapLaxmikant RathiNo ratings yet
- Artifact Recognition and Troubleshooting Focus 2017Document59 pagesArtifact Recognition and Troubleshooting Focus 2017Hernán MarínNo ratings yet
- Medical Surgical Drug StudyDocument45 pagesMedical Surgical Drug StudyMichelle Angela AlombroNo ratings yet
- PhysioEx Exercise 6 Activity 5Document4 pagesPhysioEx Exercise 6 Activity 5MARILYN MARIANA HERNANDEZ MENDOZANo ratings yet
- BTLS Primary Survey GuideDocument24 pagesBTLS Primary Survey GuideJecky CazorhaNo ratings yet
- Dela Peña NCP 3Document2 pagesDela Peña NCP 3Mark Teofilo Dela PeñaNo ratings yet
- Cardiac Cycle: DR Rida Ajmal KhanDocument29 pagesCardiac Cycle: DR Rida Ajmal KhanMooma fatimaNo ratings yet
- Decompensatedcirrhosis Andfluidresuscitation: Erin MaynardDocument6 pagesDecompensatedcirrhosis Andfluidresuscitation: Erin MaynardBruno MaiaNo ratings yet
- Healy World Certificate of Conformity en EUDocument38 pagesHealy World Certificate of Conformity en EUJOHANNA BJARNERNo ratings yet
- Physical DimensionDocument5 pagesPhysical DimensionEddie AlcazarNo ratings yet
- Advance Medical-Surgical Nursing Practicum 2 Clinical PaperDocument3 pagesAdvance Medical-Surgical Nursing Practicum 2 Clinical PaperXenita VeraNo ratings yet
- Maccallum 1909Document34 pagesMaccallum 1909victor mejiaNo ratings yet
- The Sleeping BrainDocument11 pagesThe Sleeping BrainGabriela Cristina García FacioNo ratings yet
- Hemostasis: Mechanisms of Blood CoagulationDocument2 pagesHemostasis: Mechanisms of Blood CoagulationAshish SrivastavaNo ratings yet
- Changan Auto - Basic First Aid TrainingDocument54 pagesChangan Auto - Basic First Aid TrainingZubair SoomroNo ratings yet
- Heart DiseasesDocument16 pagesHeart DiseasesSanaNo ratings yet
- ACS FianlDocument72 pagesACS FianlmawardikaNo ratings yet
- Principles of Anatomy and PhysiologyDocument9 pagesPrinciples of Anatomy and PhysiologyJackson JastariNo ratings yet
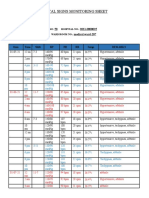
- Vital Signs Monitoring SheetDocument2 pagesVital Signs Monitoring SheetRenea Joy ArruejoNo ratings yet
- Lecture 9 Motor System 1Document33 pagesLecture 9 Motor System 1KexinNo ratings yet
- Embalming BASUGDocument39 pagesEmbalming BASUGMaryam MahmudNo ratings yet
- ABCs of ECGs: A Guide to Basic ECG InterpretationDocument67 pagesABCs of ECGs: A Guide to Basic ECG InterpretationSuresh ChevagoniNo ratings yet
- Lab-3 Toads Heart Contractile ResponseDocument4 pagesLab-3 Toads Heart Contractile ResponseWilson CheungNo ratings yet