You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Family Practice Superbill SampleDocument1 pageFamily Practice Superbill SampleRebecca Caster Fontana100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OPD 2 2019 Clinical Teaching PlanDocument3 pagesOPD 2 2019 Clinical Teaching PlanGee Ridad0% (1)
- Plastic & Reconstructive Surgery Poster PDFDocument1 pagePlastic & Reconstructive Surgery Poster PDFMZALENDO.NETNo ratings yet
- Corrective Lower Limb Osteotomies in ChiDocument7 pagesCorrective Lower Limb Osteotomies in ChiPriscilla PriscillaNo ratings yet
- Fractures of The Tibial Shaft in AdultsDocument14 pagesFractures of The Tibial Shaft in AdultsPriscilla PriscillaNo ratings yet
- Femoro-Acetabular Impingement. ClassificDocument10 pagesFemoro-Acetabular Impingement. ClassificPriscilla PriscillaNo ratings yet
- The Advantages of Circular External FixaDocument6 pagesThe Advantages of Circular External FixaPriscilla PriscillaNo ratings yet
- Taylor Spatial Frame Fixation in PatientDocument9 pagesTaylor Spatial Frame Fixation in PatientPriscilla PriscillaNo ratings yet
- WarwickAgreementonFAISyndrome BrJSportsMed 2016 Griffin 1169 76Document10 pagesWarwickAgreementonFAISyndrome BrJSportsMed 2016 Griffin 1169 76Priscilla PriscillaNo ratings yet
- Biomechanical Comparison of Dynamic Hip Screw, ProximalDocument24 pagesBiomechanical Comparison of Dynamic Hip Screw, ProximalPriscilla PriscillaNo ratings yet
- Same Same, But Different?: Should Football Boot Selection Be A Consideration After AclrDocument6 pagesSame Same, But Different?: Should Football Boot Selection Be A Consideration After AclrAleks Guevara PalaciosNo ratings yet
- Assesment Post Op Ratna GCT Radius - Preop Sekar MegaprothesisDocument32 pagesAssesment Post Op Ratna GCT Radius - Preop Sekar MegaprothesisReza Devianto HambaliNo ratings yet
- Permedica 2.semnatDocument74 pagesPermedica 2.semnatCiprian VasileNo ratings yet
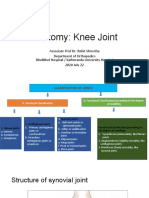
- Anatomy of KneeDocument28 pagesAnatomy of KneeManish AdhikariNo ratings yet
- Tympanoplasty - News and New PerspectivesDocument21 pagesTympanoplasty - News and New PerspectivesMonik AlamandaNo ratings yet
- The History of Neurosurgery in Bolivia and PediatrDocument7 pagesThe History of Neurosurgery in Bolivia and PediatrMarcela Sanchez ParraNo ratings yet
- DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1Document2 pagesDOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1jheanniver nablo100% (1)
- Project Information Memorandum: Medica Synergie Private LimitedDocument41 pagesProject Information Memorandum: Medica Synergie Private LimitedEyock PierreNo ratings yet
- مصطلاحات هندسية PDFDocument160 pagesمصطلاحات هندسية PDFHossam MakiNo ratings yet
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDocument4 pagesSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraNo ratings yet
- Lumbotomy - Proximal Ureterolithotomy RIUDocument22 pagesLumbotomy - Proximal Ureterolithotomy RIUDwiyanti OktaviaNo ratings yet
- Dr. Cereno and Dr. Zafe v. Court of AppealsDocument2 pagesDr. Cereno and Dr. Zafe v. Court of Appealserxha ladoNo ratings yet
- Esu-X 300 NT (CL II B CEE 93/42) : SER Anual ForDocument35 pagesEsu-X 300 NT (CL II B CEE 93/42) : SER Anual Foralejandro sanche mejoradaNo ratings yet
- Draft Space Program - Trauma CenterDocument5 pagesDraft Space Program - Trauma CenterMai MalkawiNo ratings yet
- Ankle Foot Orthosis (AFO)Document10 pagesAnkle Foot Orthosis (AFO)aienjalilNo ratings yet
- Transdisciplinary Clinical Practice Between Physiotherapists and Traumatologists in Orthopaedic MedicineDocument9 pagesTransdisciplinary Clinical Practice Between Physiotherapists and Traumatologists in Orthopaedic MedicineEnrique LopezNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormsalescoordinatorNo ratings yet
- Assisstive DevicesDocument45 pagesAssisstive DevicesNaveen Kumar100% (1)
- Bilateral Macrostomia: Interesting Case SeriesDocument4 pagesBilateral Macrostomia: Interesting Case Seriesahmed bouzouidaNo ratings yet
- Caring of Client With Immobilization DevicesDocument6 pagesCaring of Client With Immobilization DevicesJmarie Brillantes PopiocoNo ratings yet
- Orthopedic Hardware in Trauma - A Guided Tour For The Radiologist - Part 1Document15 pagesOrthopedic Hardware in Trauma - A Guided Tour For The Radiologist - Part 1Marcia MejíaNo ratings yet
- Artikel BunionDocument6 pagesArtikel BunionIsmi SyafitriNo ratings yet
- DoctorsDocument15 pagesDoctorsRitu MishraNo ratings yet
- Physiotherapy DepartmentDocument5 pagesPhysiotherapy DepartmentkaushikawebNo ratings yet
- Revision StapedectomyDocument21 pagesRevision Stapedectomyapi-19500641100% (1)
- Doctor Mahavir EnclaveDocument22 pagesDoctor Mahavir EnclaveFortune BuildersNo ratings yet
- DR LegaspiDocument6 pagesDR LegaspijheyfteeNo ratings yet