You might also like
- MEDADV Radiology Cardiology Guidelines 3 1 2021 PDFDocument1,905 pagesMEDADV Radiology Cardiology Guidelines 3 1 2021 PDFAy ohNo ratings yet
- Standards For Diagnostic RadiologyDocument25 pagesStandards For Diagnostic Radiologymohadese EstajiNo ratings yet
- Clinical Anatomy of The Shoulder An Atlas PDFDocument98 pagesClinical Anatomy of The Shoulder An Atlas PDFSylvinho46100% (1)
- Roh2201123544 2Document3 pagesRoh2201123544 2Ruby kushwahNo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- Emergency Medicine in MBBSDocument85 pagesEmergency Medicine in MBBSPATHMAPRIYA GANESANNo ratings yet
- Medical Device Regulation-USFDADocument38 pagesMedical Device Regulation-USFDAMADDINENI AVANEESHWARNo ratings yet
- Focused Reviews: Bronchoscopic CryotherapyDocument11 pagesFocused Reviews: Bronchoscopic CryotherapyNEUMOLOGIA HNGAINo ratings yet
- Jeevan Suraksha Hospital 1-2Document25 pagesJeevan Suraksha Hospital 1-2Tarun KumarNo ratings yet
- Kidney Stone Disease Say NO To Stones - 1st PDFDocument247 pagesKidney Stone Disease Say NO To Stones - 1st PDFIosub Lica-ClaudiuNo ratings yet
- Vascular Neurology Board Review: An Essential Study GuideFrom EverandVascular Neurology Board Review: An Essential Study GuideHardik P. AminRating: 4 out of 5 stars4/5 (1)
- Indwelling Urinary CatheterizationDocument8 pagesIndwelling Urinary CatheterizationNiña Jean Tormis AldabaNo ratings yet
- CT RequestDocument1 pageCT Requestraad_alghamdi_1No ratings yet
- Mri Request FormDocument2 pagesMri Request Formraad_alghamdi_1No ratings yet
- نموذج انقاذ حياة الجديدDocument2 pagesنموذج انقاذ حياة الجديدraad_alghamdi_1No ratings yet
- تحويل عبد الرحمن زايدDocument1 pageتحويل عبد الرحمن زايدraad_alghamdi_1No ratings yet
- تحويل سعد الصانعDocument1 pageتحويل سعد الصانعraad_alghamdi_1No ratings yet
- تحويل احمد السبرDocument2 pagesتحويل احمد السبرraad_alghamdi_1No ratings yet
- نموذج تحويلDocument1 pageنموذج تحويلraad_alghamdi_1No ratings yet
- Practice Full Manual-1-12Document12 pagesPractice Full Manual-1-12p7hgzmkct4No ratings yet
- PT Referral 1Document1 pagePT Referral 1raad_alghamdi_1No ratings yet
- Cardiac Silhouette Is Normal. Rib Cage Appears NormalDocument2 pagesCardiac Silhouette Is Normal. Rib Cage Appears Normalsumit1234ggNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- U.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Document17 pagesU.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Fabrício Rios Moreira100% (1)
- YSF210769689Document2 pagesYSF210769689ayushNo ratings yet
- GOS18 Referral Form 1Document2 pagesGOS18 Referral Form 1parvathyNo ratings yet
- RCC Northwest Patient Referral Form Dec2017 - FINALDocument2 pagesRCC Northwest Patient Referral Form Dec2017 - FINALkelvinwinfordNo ratings yet
- PL0009Document2 pagesPL0009mukundj46No ratings yet
- Singlife - Pre-Hospitalisation Form (PHF) - 2023Document1 pageSinglife - Pre-Hospitalisation Form (PHF) - 2023shemanth123No ratings yet
- Frontal Radiograph Chest (Pa View) FindingsDocument2 pagesFrontal Radiograph Chest (Pa View) Findingsmdsiraj16150No ratings yet
- Ministry of Health Directorate of Health Affairs - Najran Maternity & Children's Hospital نارجن - ةيحصلا نوؤشلا ةيريدم لافطلأاو ةدلاولا ىفشتسمDocument2 pagesMinistry of Health Directorate of Health Affairs - Najran Maternity & Children's Hospital نارجن - ةيحصلا نوؤشلا ةيريدم لافطلأاو ةدلاولا ىفشتسمSaifeldein ElimamNo ratings yet
- Referral FormDocument2 pagesReferral Formraad_alghamdi_1No ratings yet
- MRI Safety Screening Questionnaire OutpatientDocument2 pagesMRI Safety Screening Questionnaire OutpatientChristian David ChicaNo ratings yet
- Form Medical Malpractice Insurance enDocument2 pagesForm Medical Malpractice Insurance ensyed imdadNo ratings yet
- Application For LicenseDocument12 pagesApplication For Licensemuhammad saqib jabbarNo ratings yet
- Courtney Broton Job33-Form3Document1 pageCourtney Broton Job33-Form3api-550569140No ratings yet
- Application For LicenseDocument11 pagesApplication For LicenseSadaf RizwanhumayoonNo ratings yet
- BD 18 April 2021Document30 pagesBD 18 April 2021Mohamad NofalNo ratings yet
- Radiology Request Form - CDRDocument2 pagesRadiology Request Form - CDRsaranyaNo ratings yet
- Abdominal PainDocument13 pagesAbdominal PainSuhair F DiebesNo ratings yet
- Pediatric Surgery Zimbabwe.Document7 pagesPediatric Surgery Zimbabwe.Thomas MutanikwaNo ratings yet
- U.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Document42 pagesU.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Mohammed SairawanNo ratings yet
- Immunology Report: Kamnath Market, Hospital Road, Lakhimpur Phone: 05872-278735, 9235400943Document1 pageImmunology Report: Kamnath Market, Hospital Road, Lakhimpur Phone: 05872-278735, 9235400943Ashutosh SinghNo ratings yet
- Laboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesDocument5 pagesLaboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesCaissa Andrea Beatrice BaylenNo ratings yet
- UHS Pre-Enrolment Med Clearance - FinalDocument3 pagesUHS Pre-Enrolment Med Clearance - FinalMikayla DutingNo ratings yet
- Medical Provider Application FormDocument4 pagesMedical Provider Application FormOmar SalhaniNo ratings yet
- Rajindra Hospital, Patiala: (Manual - 1) Particulars of Organization, Functions and DutiesDocument2 pagesRajindra Hospital, Patiala: (Manual - 1) Particulars of Organization, Functions and DutiesJs KalerNo ratings yet
- Out Patient Department (OPD) Cashless Card-BenefitsDocument10 pagesOut Patient Department (OPD) Cashless Card-BenefitsHemantNo ratings yet
- APSC Fellowship Application 2014aDocument5 pagesAPSC Fellowship Application 2014aFahmi RaziNo ratings yet
- PT Referral 2Document1 pagePT Referral 2raad_alghamdi_1No ratings yet
- Citizen CharterDocument10 pagesCitizen Charterganeshgupta1432.ggNo ratings yet
- SR - Adverticement - New - Organized-3 (1) - 240212 - 163242Document6 pagesSR - Adverticement - New - Organized-3 (1) - 240212 - 163242Hitendra GuptaNo ratings yet
- F09. Plan FormDocument5 pagesF09. Plan Formahmed salahNo ratings yet
- LetterHead Official - Public-English Ver INDRLsDocument8 pagesLetterHead Official - Public-English Ver INDRLsFISICO CADAVIDNo ratings yet
- Book No MLC No Hospital NameDocument6 pagesBook No MLC No Hospital NameUmair KhaliqNo ratings yet
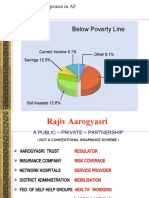
- Hospitalization Expenses in APDocument10 pagesHospitalization Expenses in APSantosh GunduNo ratings yet
- Hospital Transfer PoliceDocument4 pagesHospital Transfer PoliceMahmoud NaggarNo ratings yet
- Tool 3 For Adapting and PrintingDocument1 pageTool 3 For Adapting and PrintingAddisNo ratings yet
- Care Plan TemplateDocument12 pagesCare Plan TemplateemipNo ratings yet
- Article 63804Document42 pagesArticle 63804AniNo ratings yet
- Vincent Attachment RportDocument20 pagesVincent Attachment Rportkimkevo12No ratings yet
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Document9 pagesMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinNo ratings yet
- 1 s2.0 S0104001421003420 MainDocument6 pages1 s2.0 S0104001421003420 MainSYAIFUL PRATAMANo ratings yet
- Report ViewerDocument1 pageReport ViewerZeeshan JunejoNo ratings yet
- Abdominal Ultrasound: Sherifa Ahmed Name Sunday, May 17, 2020, 13:58 A5/p5 Date 3753 MRNDocument1 pageAbdominal Ultrasound: Sherifa Ahmed Name Sunday, May 17, 2020, 13:58 A5/p5 Date 3753 MRNrizwan qureshiNo ratings yet
- Referral FormDocument2 pagesReferral Formraad_alghamdi_1No ratings yet
- نموذج فرز الاعراض التنفسيةDocument1 pageنموذج فرز الاعراض التنفسيةraad_alghamdi_1No ratings yet
- تحويل المريض حسين الحسينDocument1 pageتحويل المريض حسين الحسينraad_alghamdi_1No ratings yet
- نموذج فرز الاعراض التنفسيةDocument1 pageنموذج فرز الاعراض التنفسيةraad_alghamdi_1No ratings yet
- تحويل احمد السبرDocument2 pagesتحويل احمد السبرraad_alghamdi_1No ratings yet
- psych. medical report بنيدرDocument4 pagespsych. medical report بنيدرraad_alghamdi_1No ratings yet
- نموذج فرز الاعراض التنفسيةDocument1 pageنموذج فرز الاعراض التنفسيةraad_alghamdi_1No ratings yet
- Ikhaa Patient RecordDocument12 pagesIkhaa Patient Recordraad_alghamdi_1No ratings yet
- Filtered AttachmentsDocument1 pageFiltered Attachmentsraad_alghamdi_1No ratings yet
- List of Long Stay Patient in HospitalDocument6 pagesList of Long Stay Patient in Hospitalraad_alghamdi_1No ratings yet
- Referral FormDocument2 pagesReferral Formraad_alghamdi_1No ratings yet
- PT Referral 2Document1 pagePT Referral 2raad_alghamdi_1No ratings yet
- REFERRAL FORM OldDocument2 pagesREFERRAL FORM Oldraad_alghamdi_1No ratings yet
- Patient StatmentDocument1 pagePatient Statmentraad_alghamdi_1No ratings yet
- URGENT CASES Old2Document1 pageURGENT CASES Old2raad_alghamdi_1No ratings yet
- Opd Progress Note PsychatricDocument1 pageOpd Progress Note Psychatricraad_alghamdi_1No ratings yet
- OPD SheetDocument3 pagesOPD Sheetraad_alghamdi_1No ratings yet
- Referral FormDocument1 pageReferral Formraad_alghamdi_1No ratings yet
- URGENT CASES Old2Document1 pageURGENT CASES Old2raad_alghamdi_1No ratings yet
- X - Ray Request & Report FormDocument1 pageX - Ray Request & Report Formraad_alghamdi_1No ratings yet
- URGENT CASES Old2Document1 pageURGENT CASES Old2raad_alghamdi_1No ratings yet
- VBA-21-0960A-2-ARE Artery and Vein PDFDocument5 pagesVBA-21-0960A-2-ARE Artery and Vein PDFCombat CraigNo ratings yet
- MIS Conical Connection Prosthetic OptionsDocument56 pagesMIS Conical Connection Prosthetic Optionsadi033No ratings yet
- Sarjina Hossain ReanDocument2 pagesSarjina Hossain ReanYousuf SawdagorNo ratings yet
- Prosthodontic Stents: March 2016Document25 pagesProsthodontic Stents: March 2016Arun PrasadNo ratings yet
- Post-Operative Instructions: Hip Hemiarthroplasty: Wound CareDocument3 pagesPost-Operative Instructions: Hip Hemiarthroplasty: Wound CareAbdullah AzmyNo ratings yet
- Clin Adv Periodontics - 2022 - Velasquez Plata - Osseous Topography in Biologically Driven Flap Design in MinimallyDocument5 pagesClin Adv Periodontics - 2022 - Velasquez Plata - Osseous Topography in Biologically Driven Flap Design in Minimally安西 泰規No ratings yet
- Or JournalDocument2 pagesOr JournalNathaniel PulidoNo ratings yet
- Operating Room Technique Write Up PAPA SLRCDocument43 pagesOperating Room Technique Write Up PAPA SLRCShane Vlademier ParadoNo ratings yet
- Surgery Surgical Nursing Objs With AnsDocument136 pagesSurgery Surgical Nursing Objs With AnsmintahmeshackbenjaminNo ratings yet
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 pagesLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneNo ratings yet
- New Consolidated List of EmpanelmentDocument36 pagesNew Consolidated List of EmpanelmentSHAURYA VERMANo ratings yet
- Introducere 1Document11 pagesIntroducere 1Victor EnachiNo ratings yet
- Chapter 7 - Technology Transfer in Health CareDocument10 pagesChapter 7 - Technology Transfer in Health CareLalita A/P AnbarasenNo ratings yet
- 2023 Vein AnatomyDocument6 pages2023 Vein AnatomyKarenNo ratings yet
- Excel ICU Logbook V1.6Document23 pagesExcel ICU Logbook V1.6aboshima739No ratings yet
- Management of Distal Radius Fractures - Treatment Protocol and Functional ResultsDocument7 pagesManagement of Distal Radius Fractures - Treatment Protocol and Functional Resultslex salomNo ratings yet
- 7th Kent ENdoscopy Training Hybrid Course Registration ProgrammeDocument3 pages7th Kent ENdoscopy Training Hybrid Course Registration ProgrammeJustine OyanibNo ratings yet
- A - Pratic Guide Pediatric Wound CareDocument9 pagesA - Pratic Guide Pediatric Wound CareLicia GabrielleNo ratings yet
- Roblin HealyDocument6 pagesRoblin HealyMiguel JohnsonNo ratings yet
- RA 7885 RA 7170 Organ Donation ActDocument41 pagesRA 7885 RA 7170 Organ Donation ActEMMANUEL CHARLES ADRIAN BAUTISTANo ratings yet
- (123doc) - Tai-Lieu-Toefl-Cbt-Book-Part-30Document10 pages(123doc) - Tai-Lieu-Toefl-Cbt-Book-Part-30Quỳnh TrâmNo ratings yet
- Doehle-Philman Manning Agency, Inc. Doehle (IOM) Limited and Capt. Manolo T. Gacutan vs. Jose N. Gatchalian, JR., G.R. No. 207507, February 17, 2021Document11 pagesDoehle-Philman Manning Agency, Inc. Doehle (IOM) Limited and Capt. Manolo T. Gacutan vs. Jose N. Gatchalian, JR., G.R. No. 207507, February 17, 2021Anonymous oGfAqF1No ratings yet
- Sop Sop English Web PDFDocument20 pagesSop Sop English Web PDFRadu TudorNo ratings yet
- Bab 84 Meckel's DivertikulumDocument8 pagesBab 84 Meckel's DivertikulumDede IskandarNo ratings yet
- Summary:: ObjectiveDocument4 pagesSummary:: Objectiverodney subaranNo ratings yet