Professional Documents
Culture Documents
Rosuvastatin A Review of Its Use in The.5
Uploaded by
urbanincultureOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Rosuvastatin A Review of Its Use in The.5
Uploaded by
urbanincultureCopyright:
Available Formats
ADIS DRUG EVALUATION
Am J Cardiovasc Drugs 2010; 10 (6): 383-400 1175-3277/10/0006-0383/$49.95/0
2010 Adis Data Information BV. All rights reserved.
Rosuvastatin
A Review of its Use in the Prevention of Cardiovascular Disease in Apparently Healthy Women or Men with Normal LDL-C Levels and Elevated hsCRP Levels
Natalie J. Carter
Adis, a Wolters Kluwer Business, Auckland, New Zealand
Various sections of the manuscript reviewed by: M.J. Banach, Department of Cardiology, Medical University of Lodz, Lodz, Poland; L. Masana, Lipid Research Unit, Sant Joan University Hospital, Reus, Spain; B. Pitt, Division of Cardiology, University of Michigan Hospital, Ann Arbor, Michigan, USA; B. Tomlinson, Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Shatin, Hong Kong; N.D. Wong, UCI Heart Disease Prevention Program, University of California at Irvine, Irvine, California, USA.
Data Selection Sources: Medical literature published in any language since 1980 on rosuvastatin, identified using MEDLINE and EMBASE, supplemented by AdisBase (a proprietary database). Additional references were identified from the reference lists of published articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug. Search strategy: MEDLINE, EMBASE and AdisBase search terms were rosuvastatin and (c-reactive or c-reactive-protein or CRP or prevention). Searches were last updated 8 September 2010. Selection: Studies in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels who received rosuvastatin. Inclusion of studies was based mainly on the methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred. Relevant pharmacodynamic and pharmacokinetic data are also included. Index terms: rosuvastatin, cardiovascular disease prevention, hsCRP, pharmacodynamics, pharmacokinetics, therapeutic use, tolerability.
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384 2. Pharmacodynamic Profile . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385 2.1 Mechanism of Action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385 2.2 Lipid and Anti-Inflammatory Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385 2.3 Other Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386 2.4 Special Populations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386 2.5 Pharmacodynamic Drug-Drug Interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387 3. Pharmacokinetic Profile . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387 3.1 Absorption and Distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387 3.2 Metabolism and Elimination. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387 3.3 Special Patient Populations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387 3.4 Pharmacokinetic Drug-Drug Interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 388 4. Therapeutic Efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 388 4.1 Primary Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 389 4.1.1 Cardiovascular Events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 389 4.1.2 Thromboembolic Events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 390 4.2 Secondary Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 391 4.2.1 Stratification According to On-Treatment Laboratory Measures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 391 4.2.2 Stratification According to Baseline Factors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 391 5. Tolerability. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 393 6. Dosage and Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395
384
Carter
7. Place in the Prevention of Cardiovascular Disease in Apparently Healthy Women or Men with Normal LDL-C Levels and Elevated hsCRP Levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395
Abstract
Rosuvastatin (Crestor) is an HMG-CoA reductase inhibitor (statin) that has both lipid-lowering and antiinflammatory effects. The drug has various indications in the US, including the primary prevention of cardiovascular disease (CVD) in patients with no clinical evidence of coronary heart disease who are at increased risk of CVD based on their age, a high-sensitivity C-reactive protein (hsCRP) level of 2 mg/L, and at least one other CVD risk factor. The efficacy of rosuvastatin in apparently healthy women (aged 60 years) or men (aged 50 years) with normal low-density lipoprotein cholesterol (LDL-C) levels and elevated hsCRP levels was demonstrated in the large, randomized, double-blind, multinational, JUPITER trial. Relative to placebo, rosuvastatin 20 mg once daily for a median follow-up of 1.9 years significantly reduced the occurrence of first major cardiovascular events in this trial (primary endpoint). A between-group difference in favor of rosuvastatin was also demonstrated for various other endpoints, including overall deaths and the nonatherothrombotic endpoint of venous thromboembolism. Rosuvastatin remained more effective than placebo when primary endpoint results were stratified according to various baseline factors, including in patient subgroups thought to be at low risk of CVD. In addition, rosuvastatin was associated with reductions in LDL-C and hsCRP levels, and these reductions appeared to occur independently of each other. The greatest clinical benefit was observed in rosuvastatin recipients achieving an LDL-C level of <1.8 mmol/L (<70 mg/dL) and an hsCRP level of <2 mg/L or, even more so, <1 mg/L. Rosuvastatin was well tolerated in the JUPITER trial, with most adverse events being mild to moderate in severity. Myalgia, arthralgia, constipation, and nausea were the most commonly occurring treatmentrelated adverse events, and the incidence of monitored adverse events and laboratory measurements was generally similar in the rosuvastatin and placebo groups. It is not yet known whether the mechanism of benefit of rosuvastatin is via lipid effects, anti-inflammatory effects, or a mixture of both, and the use of rosuvastatin solely on the basis of elevated hsCRP levels is controversial. Nonetheless, the drug remains an important pharmacologic option in the prevention of CVD, and has demonstrated efficacy in preventing major cardiovascular events in apparently healthy women (aged 60 years) or men (aged 50 years) with normal LDL-C levels and elevated hsCRP levels.
1. Introduction Cardiovascular disease (CVD) is the leading cause of death in the US, with more people dying each year from CVD than from cancer, chronic lower respiratory tract diseases, and accidents combined.[1] The term CVD encompasses a wide range of cardiovascular-related diseases, including hypertension, coronary heart disease (CHD) [i.e. myocardial infarction (MI) or angina pectoris], heart failure, stroke, and congenital cardiovascular defects.[1] The risk of developing CVD increases with age, and the disease is more common in men than in women in younger age groups, although this difference disappears with advancing age.[1] By 40 years of age, the lifetime risk of developing CVD is >1 in 2 for women, and 2 in 3 for men.[1] Overall, an estimated 81 million adults in the US have one or more types of CVD at any given time, with >38 million of these adults being aged 60 years.[1] The risk of developing CVD is commonly assessed using the Framingham risk model (or a variation of this model), with patients being stratified into low- (10-year risk <10%), intermediate- (10-year risk 1020%), or high- (10-year risk >20%)
2010 Adis Data Information BV. All rights reserved.
risk groups according to age, sex, systolic blood pressure, serum total cholesterol level, high-density lipoprotein cholesterol (HDL-C) level, and whether or not they smoke; diastolic blood pressure, low-density lipoprotein cholesterol (LDL-C) level, a family history of premature CHD, and/or a history of diabetes mellitus is also taken into account in some instances.[2-4] However, a proportion of patients considered to be at low risk of CVD based on these traditional risk factors will go on to develop CVD (section 7).[5,6] Therefore, identification of other factors that may enable physicians to identify more patients at risk of CVD is of interest,[3,6] particularly those that enable reclassification of intermediate-risk patients as either low- or high-risk.[3] HMG-CoA-reductase inhibitors (statins) are lipid-lowering agents that are recommended in current US guidelines as firstline treatment options for the pharmacologic lowering of LDL-C levels.[2,4] In clinical trials, some of these drugs also had beneficial effects on inflammatory biomarkers (e.g. C-reactive protein [CRP] levels) in patients with dyslipidemia, including those at high-risk of developing CVD and those with established CVD (section 2.2).[7] Moreover, these anti-inflammatory
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
385
effects were associated with clinical benefits that were independent of those associated with changes in the lipid profile in patients with stable CVD or acute coronary syndrome (section 2.2).[8-13] Based on findings from these and other trials, it was postulated that high-sensitivity CRP levels (i.e. CRP levels measured with a high-sensitivity assay [hsCRP]) may be of use as an additional marker of CVD risk.[14,15] Rosuvastatin (Crestor) is one of the statins for which antiinflammatory effects have been demonstrated in dyslipidemic patients (section 2.2) [reviewed by Keating and Robinson[7]]. To further explore the relationship between rosuvastatin-associated reductions in hsCRP and CVD prevention, the efficacy of the drug was investigated in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels in the pivotal JUPITER (Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial.[15] Subsequent to the favorable results observed in this trial (section 4),[15] the approved indications of rosuvastatin in the US were expanded to include the primary prevention of CVD in patients with no clinical evidence of CHD, who are at increased risk of CVD based on their age, an hsCRP level of 2 mg/L, and the presence of at least one other CVD risk factor (section 6).[16] The drug is also indicated for the management of various dyslipidemias and to slow the progression of atherosclerosis (section 6).[16] The use of rosuvastatin in the management of dyslipidemia[17,18] or to slow the prevention of atherosclerosis[7] has been reviewed previously. This article specifically focuses, from a US perspective, on the use of rosuvastatin in the prevention of CVD in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels, as well as reviewing aspects of its pharmacologic properties and tolerability that are relevant to this population of patients. Where data are unavailable in the main patient population, key information from studies in other patient populations are provided. 2. Pharmacodynamic Profile
2.1 Mechanism of Action
2.2 Lipid and Anti-Inflammatory Effects
As for all statins, rosuvastatin is an inhibitor of HMG-CoA reductase, an enzyme involved in the pathway leading to the generation of cholesterol.[7] Rosuvastatin is relatively hydrophilic and is highly selective for hepatic cells.[7] The uptake of rosuvastatin into the liver is mediated by organic anion-transporting polypeptide (OATP)-1B1 (formerly OATP-C), a liverspecific transport protein.[19] Rosuvastatin is a high-affinity substrate for OATP-1B1, and has a higher affinity for this transport protein than other statins.[7]
2010 Adis Data Information BV. All rights reserved.
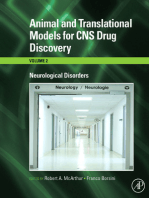
The pharmacologic effects of rosuvastatin in patients with hypercholesterolemia and/or other dyslipidemias (including high-risk patients and special patient populations) with or without CVD have been well described previously.[7,17,18] In brief, rosuvastatin decreased LDL-C levels by up to 57%, and to recommended goals in up to 84% (National Cholesterol Education Program [NCEP] Adult Treatment Panel [ATP] III goals) or 89% (Joint European Societies 1998 goals) of patients in clinical trials (reviewed by Keating and Robinson[7]). In general, total cholesterol, triglyceride, and apolipoprotein (apo) B levels were decreased, and HDL-C and apoA1 levels were increased by the drug.[7] In addition to its beneficial effects on the lipid profile, rosuvastatin also demonstrated anti-inflammatory properties in this population of patients by decreasing CRP, fibrinogen, and proinflammatory cytokine levels.[7] Similar improvements in inflammatory parameters have been observed in patients with stable CVD or acute coronary syndrome, and these improvements were associated with clinical benefits that were independent of those associated with changes in the lipid profile (section 1).[8-13] In general, rosuvastatin 540 mg/day for 624 weeks was as effective or more effective (p < 0.05) than other statins (atorvastatin 1080 mg/day, pravastatin 1040 mg/day, and/or simvastatin 1080 mg/day) in decreasing LDL-C, total cholesterol, apoB, or CRP levels in patients with hypercholesterolemia (and/or other dyslipidemias) with or without CVD, with some between-group differences in favor of rosuvastatin also being demonstrated for changes in HDL-C, apoA1, and, less frequently, triglyceride levels (reviewed by Keating and Robinson[7]). Rosuvastatin also demonstrated beneficial lipid-lowering and anti-inflammatory effects in patients with normal LDL-C levels (<3.4 mmol/L [<130 mg/dL]) and elevated hsCRP (2.0 mg/L) levels in the pivotal JUPITER trial.[15] Relative to baseline measurements, median hsCRP levels were decreased by 4857%, median LDL-C levels by 4951%, and median triglyceride levels by 1016% after treatment with rosuvastatin 20 mg once daily for 12, 24, 36, or 48 months (figure 1). Rosuvastatin also increased median HDL-C levels by 26% over the same treatment period (figure 1).[15] Aside from median HDL-C levels at 48 months, which were similar in both the rosuvastatin and placebo groups, all other between-group differences in hsCRP, LDL-C, triglyceride, and HDL-C levels were significantly (p 0.003) in favor of rosuvastatin at all timepoints (figure 1).[15] Furthermore, rosuvastatin-related reductions in LDL-C and hsCRP levels were associated with clinical benefit in the JUPITER trial, particularly when both parameters were reduced
Am J Cardiovasc Drugs 2010; 10 (6)
386
Carter
a 5.0 4.5 4.0 hsCRP (mg/L) 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 c 2.0 2.0 0 ** ** ** ** LDL-C (mmol/L) 2.5 2.0 1.5 1.0 0.5 3.0
ROS PL
**
**
**
**
HDL-C (mmol/L)
1.5
1.5 TG (mmol/L) ** ** * ** 1.0 ** ** **
1.0
0.5
0.5
0 Baseline 12 mo 24 mo 36 mo 48 mo
0 Baseline 12 mo 24 mo 36 mo 48 mo
Fig. 1. Pharmacologic effects of rosuvastatin (ROS) in patients (pts) with normal low-density lipoprotein-cholesterol (LDL-C) levels and elevated highsensitivity C-reactive protein (hsCRP) levels. Median (a) hsCRP, (b) LDL-C, (c) high-density lipoprotein-cholesterol (HDL-C), and (d) triglyceride (TG) levels at baseline and after 12, 24, 36, or 48 months of treatment with ROS 20 mg or placebo (PL) once daily in the JUPITER trial. * p = 0.003, ** p < 0.001 vs PL.
to below predetermined goals (i.e. <1.8 mmol/L [<70 mg/dL]) for LDL-C levels and <1 or <2 mg/L for hsCRP levels) [section 4.2.1].[15]
2.3 Other Effects
thrombin receptor on platelets isolated from rosuvastatin-treated patients with metabolic syndrome.[7]
2.4 Special Populations
As reviewed previously, rosuvastatin has demonstrated many other pharmacodynamic effects in in vitro, animal, and clinical studies. For example, in patients with hypercholesterolemia or CVD, rosuvastatin decreased plasma asymmetric dimethylarginine levels, improved flow-mediated dilation, increased paroxonase-1 activity, decreased levels of oxidative stress markers, and attenuated the postprandial rise in platelet count.[7] In murine models of carotid artery injury, platelet aggregation and the endothelial injury-related thrombotic response were attenuated, vascular lesion development and fibrin deposition were decreased, re-endothelialization was promoted, and smooth muscle cell and collagen content were increased after treatment with rosuvastatin.[7] Furthermore, expression of CD40 and metalloproteinase (MMP) was inhibited by rosuvastatin in apoE knockout mice, and this effect was increased when rosuvastatin was coadministered with candesartan.[7] In addition, rosuvastatin reduced the in vitro secretion of MMP-7 in human monocyte-derived macrophages and inhibited the expression of protease-activated receptor-1
2010 Adis Data Information BV. All rights reserved.
[7]
LDL-C levels were decreased in a gene-dose dependent manner in Chinese patients with hypercholesterolemia[20,21] and in post-MI patients[22] (>96% European Caucasian[23]) who received rosuvastatin for at least 4 weeks in clinical studies. Of all the polymorphisms genotyped in one of the Chinese studies, genetic variability in the gene encoding for ATP-binding cassette G2 protein (an efflux transporter) was most highly associated with this gene-dose response.[21] In the Chinese studies, patients who were homozygous for the c.421A variant allele (c.421AA genotype; n = 39[20] and 55[21]) had a significantly (p 0.0006) greater percent change in LDL-C levels from baseline to endpoint than those who were homozygous for the wild-type allele (c.421CC genotype; n = 158[20] and 191[21]) [-57%[20,21] vs -49%[21] and -50%[20]]. Chinese patients who were heterozygous for the c.421A variant allele (c.421AC genotype; n = 108[20] and 136[21]) had an intermediate response to rosuvastatin therapy (percent change in LDL-C levels of -54%[20,21]). Similar findings were seen in the European Caucasian study, with a significant (p = 0.01) difference being observed in 3-month LDL-levels between patients with the
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
387
c.421CC genotype (n = 231) and those with either the c.421AA or c.421AC genotype (n = 79) [2.0 vs 1.8 mmol/L (76 vs 68 mg/dL)].[22] Pharmacokinetic data discussed in section 3.3 are reflective of these results.
2.5 Pharmacodynamic Drug-Drug Interactions
Coadministration of rosuvastatin with other lipid-lowering drugs (e.g. fibric acid derivatives [e.g. fenofibrate, gemfibrozil] or niacin), cyclosporine (ciclosporin), atazanavir/ritonavir, or lopinavir/ritonavir may increase the risk of developing myopathy.[16] Because of this, although concomitant use of rosuvastatin and fenofibrate did not alter the pharmacokinetics of either drug to a clinically relevant extent (section 3.4), the manufacturers prescribing information recommends reducing the dose of rosuvastatin when the two drugs are combined.[16] For similar reasons, a reduction in rosuvastatin dose should be considered if the drug is administered in conjunction with niacin.[16] Rosuvastatin increased the anticoagulant effect of warfarin in healthy volunteers and in patients who received the drugs concomitantly (section 3.4).[24] In patients already receiving warfarin, the international normalized ratio should be determined prior to initiating treatment with rosuvastatin, and should continue to be monitored frequently during the initial concomitant treatment period.[16] 3. Pharmacokinetic Profile The pharmacokinetics of rosuvastatin have not been specifically studied in healthy women or men with normal LDL-C levels and elevated hsCRP. This section provides an overview of the pharmacokinetics of rosuvastatin in healthy volunteers or other populations of patients, which have been reviewed elsewhere.[7,17,18]
3.1 Absorption and Distribution
of day at which the drug was administered,[27] and administration with (as opposed to without) food did not alter the pharmacokinetics to a clinically relevant extent.[16] Rosuvastatin is 88% bound to plasma proteins, mainly albumin.[16] The estimated volume of distribution at steady state is 134 L, indicating that the drug is widely distributed to the tissues.[26] As demonstrated by a >70% rate of nonrenal clearance and a high hepatic extraction ratio (section 3.2), it appears that rosuvastatin is distributed extensively into the human liver.[26]
3.2 Metabolism and Elimination
In healthy volunteers, rosuvastatin demonstrated linear, dosedependent increases in the geometric mean maximum plasma concentration (3.810.3 ng/mL) [Cmax] and the mean area under the plasma concentration-time curve (AUC) from time zero to the last measurable concentration (31.698.2 ng h/mL) [AUClast] over a dose range of 1040 mg.[25] The AUC from time zero to 24 hours also increased with rosuvastatin dose (30.784.4 ng h/mL); however, the median time to Cmax (5.0 hours) was not dose dependent.[25] The estimated absolute oral bioavailability of rosuvastatin after a single oral 40 mg dose was 20%.[26] Steady-state concentrations were achieved by the eighth day of treatment with rosuvastatin 10 mg once daily.[27] The pharmacokinetics of rosuvastatin were not affected by the time
The primary elimination route of rosuvastatin is via the liver.[28] Because of its low bioavailability and high hepatic extraction ratio of 0.63, the drug is thought to undergo firstpass metabolism.[26] Rosuvastatin may also undergo enterohepatic recirculation, as demonstrated by secondary peaks in individual plasma concentration-time profiles.[25,26,28] Rosuvastatin is not extensively metabolized,[29] and the cytochrome P450 (CYP) system plays only a minor role in its metabolism.[29,30] CYP2C9 is the main CYP isozyme involved in the small proportion of rosuvastatin metabolism that occurs via the CYP system; CYP3A4 does not contribute to this process.[29,30] The HMG-CoA reductase inhibitory activity of N-desmethyl rosuvastatin (the major metabolite of rosuvastatin) is about one-sixth to one-half that of the parent drug.[16] In healthy volunteers, excretion of a single radiolabelled dose of rosuvastatin was complete after 240 hours.[28] Approximately 90% of the dose was excreted in the feces (70% of the radioactive dose within 2472 hours), and the remainder in the urine.[28] Unchanged drug accounted for the majority (77%) of the total administered dose recovered in the feces, and the two rosuvastatin metabolites identified accounted for 6% and 2%.[28] The geometric mean plasma clearance of rosuvastatin 8 mg after a single intravenous dose was 48.9 L/h.[26] Approximately 28% of total body clearance occurs via the renal route, with at least 90% of this being accounted for by net tubular secretion;[26] the remainder of total body clearance occurs via the hepatic route.[16] Rosuvastatin plasma concentrations decreased in a biphasic manner after oral administration, first during the distribution phase (up to 18 hours), and then during a longer terminal elimination phase.[25,28] After a single oral dose of rosuvastatin 40 mg, the mean terminal elimination half-life was 20 hours.[26]
3.3 Special Patient Populations
Age and sex did not alter the pharmacokinetics of rosuvastatin to a clinically relevant extent.[31] However, rosuvastatin
Am J Cardiovasc Drugs 2010; 10 (6)
2010 Adis Data Information BV. All rights reserved.
388
Carter
geometric mean AUClast and Cmax values were 2-fold higher in Asian versus Caucasian patients.[32] On the basis of this finding, a reduced dose of rosuvastatin is recommended in Asian patients (section 6).[16] Exposure to rosuvastatin was affected by hepatic dysfunction, with Cmax and AUC values increasing by 60% and 5% in patients with mild (Child-Pugh class A) hepatic impairment and by 100% and 21% in those with moderate (Child-Pugh class B) hepatic impairment relative to healthy volunteers.[16] Plasma concentrations of rosuvastatin were also increased in patients with alcohol-related, chronic liver disease.[16] Because of this, rosuvastatin is contraindicated in patients with active liver disease (or unexplained persistent transaminase elevations), and should be used with caution in those with a history of chronic liver disease or excess alcohol use (section 5).[16] Renal impairment of mild or moderate (creatinine clearance [CLCR] 30 but 80 mL/min/1.73 m2) severity did not alter the pharmacokinetics of rosuvastatin.[16] However, exposure to rosuvastatin was increased by 3-fold in patients with severe renal impairment (CLCR <30 mL/min/1.73 m2) who were not receiving dialysis compared with healthy volunteers.[16] Because of this, the US prescribing information recommends commencing rosuvastatin at the lowest dose of 5 mg in patients with severe renal impairment who are not receiving hemodialysis, and that the dose is not increased to above 10 mg (section 6).[16] No dose reductions are required in those with mild or moderate renal impairment.[16] The pharmacokinetics of rosuvastatin were affected by genetic variability in the ABCG2 gene in Chinese[33] and Finnish[34] healthy volunteers. In the Finnish study, 1% of the overall study population (n = 660) had the c.421AA genotype, 17% had the c.421AC genotype, and 82% had the c.421CC genotype. In individuals with the c.421AA genotype who underwent pharmacokinetic testing (n = 4), the AUC from time zero to infinity was 100% greater than in those with the c.421AC genotype (n = 12) and 144% greater than in those with the c.421CC genotype (n = 16). In addition, the Cmax was significantly higher in healthy volunteers with the c.421AA genotype than in those with the c.421AC (108%) or c.421CC genotypes (131%). The effects of such findings on the pharmacodynamics of rosuvastatin are discussed in section 2.4.[34]
3.4 Pharmacokinetic Drug-Drug Interactions
hibitor fluconazole[38] or with the CYP2C9 substrate warfarin did not affect the pharmacokinetics of rosuvastatin.[24] The pharmacokinetics of rosuvastatin were not altered to a clinically significant extent by the lipid-lowering agents fenofibrate,[39] ezetimibe,[40] or omega-3 fatty acids (ethyl-eicosapentaenoic acid plus ethyl-docosahexaenoic acid).[41] However, coadministration with gemfibrozil increased rosuvastatin exposure by 2-fold.[42] Because of the pharmacodynamic effects this may cause (section 2.5), the US prescribing information recommends that the combination of rosuvastatin and gemfibrozil be avoided and, if the combination is indicated, that the dosage of rosuvastatin should not exceed 10 mg once daily.[16] Rosuvastatin AUC was increased by up to 3-fold and Cmax by up to 7-fold when the drug was coadministered with the atazanavir/ritonavir[43] or lopinavir/ritonavir.[44] If one of these combinations is indicated, the dosage of rosuvastatin should be limited to 10 mg once daily.[16] Rosuvastatin exposure was increased by 2-fold[45] and <1.5-fold[44] when the drug was administered with tipranavir/ritonavir[45] or fosamprenavir/ ritonavir.[44] Because of this, it is advised that such combinations are used with caution.[16] It is also recommended that the dose of rosuvastatin is limited to 5 mg when the drug is coadministered with cyclosporine,[16] because of the associated increase (AUC24 by 7-fold and Cmax by 11-fold) in rosuvastatin exposure observed when the two drugs are combined.[46] Simultaneous administration of rosuvastatin with aluminium and magnesium hydroxide antacid decreased rosuvastatin exposure by 50%; however, when the drugs were administered 2 hours apart, rosuvastatin exposure was decreased by only 20%.[47] Rosuvastatin did not alter the pharmacokinetics of digoxin,[48] cyclosporine,[46] ezetimibe,[40] or fenofibrate[39] to a clinically relevant extent, or that of ethinylestradiol or norgestimate in women receiving a combined oral contraceptive.[49] Despite the pharmacodynamic effect observed when rosuvastatin and warfarin are combined (section 2.5), the plasma concentrations of R- and S-warfarin were not altered to a clinically significant extent when the two drugs were coadministered.[24] However, it is possible that some other pharmacokinetic interaction, such as a reduced clearance of unbound R- or S-warfarin may account for the pharmacodynamic effect.[24] 4. Therapeutic Efficacy The efficacy of rosuvastatin in the prevention of CVD in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels was explored in the large (n = 17 802),
Am J Cardiovasc Drugs 2010; 10 (6)
As expected with a drug that is not metabolized by CYP3A4 (section 3.2), the pharmacokinetics of rosuvastatin were not altered by coadministration with the CYP3A4 inhibitors erythromycin,[35] ketoconazole,[36] or itraconazole.[37] In addition, coadministration with the CYP2C9 and CYP2C19 in 2010 Adis Data Information BV. All rights reserved.
Rosuvastatin: A Review
389
randomized, double-blind, placebo-controlled, multinational JUPITER trial.[50] Results discussed in this section are from primary analyses conducted in the overall patient population (section 4.1)[15,51-53] and of secondary analyses in which primary endpoint results were stratified according to various baseline (section 4.2.2)[54-59] or on-treatment (section 4.2.1) factors.[59,60] Some data are available as an abstract.[56] Additional information available in the manufacturers US prescribing information are discussed where appropriate.[16] Women aged 60 years and men aged 50 years were eligible for the JUPITER trial if they had no past medical history of CVD (i.e. MI, stroke, arterial revascularization, or other coronary risk equivalent[14]) and if they had an hsCRP level of 2.0 mg/L, an LDL-C level of <3.4 mmol/L (<130 mg/dL), and a triglyceride level of <5.65 mmol/L (<500 mg/dL).[50] Key exclusion criteria included previous or current use of any lipid-lowering therapy; current use of postmenopausal hormone replacement therapy or immunosuppressants; an ALT level >2 the upper limit of normal (ULN), a creatine kinase level >3 the ULN, a thyroid-stimulating hormone level >1.5 the ULN, and/or a creatinine level >2.0 mg/dL (150 mmol/L); a history of any nonbasal or nonsquamous cell carcinoma in the past 5 years; a history of diabetes, uncontrolled hypertension, or a chronic inflammatory condition (e.g. severe arthritis, systemic lupus erythematosus, or inflammatory bowel disease); and a recent history of drug or alcohol abuse or any other medical illness that might affect the results of the study.[50] After a 4-week run-in phase, eligible patients were randomized 1 : 1 to receive oral rosuvastatin 20 mg (n = 8901) or placebo (n = 8901) once daily for up to 5 years.[15] However, because rosuvastatin demonstrated a clear benefit over placebo in an interim efficacy analysis, the study was terminated after a median follow-up duration of 1.9 years (maximum follow-up of 5 years).[15] Results in this section pertain to the results of the interim efficacy analysis, unless otherwise specified. The primary efficacy endpoint of the JUPITER trial was the occurrence of first major cardiovascular events, which included the combined incidence of nonfatal MI, nonfatal stroke, hospitalization for unstable angina, arterial revascularization procedures, and deaths due to cardiovascular causes.[15] The incidences of each individual component of the primary efficacy endpoint were secondary endpoints,[14,15] as were the incidences of total mortality,[14,15] noncardiovascular deaths,[14] venous thromboembolism,[14] diabetes,[14] and bone fractures.[14] The frequency of newly diagnosed diabetes occurring in the JUPITER trial is discussed in section 5; data pertaining to the incidence of bone fractures are not yet available. Primary endpoint results were also stratified according
2010 Adis Data Information BV. All rights reserved.
to the hsCRP (<2 or 2 mg/L and <1 or 1 mg/L) and LDL-C level (<1.8 or 1.8 mmol/L [<70 or 70 mg/dL]) achieved at the 1-year follow-up in a prespecified analysis (section 4.2.1),[60] and according to various baseline factors in a number of post hoc analyses[54-59] (section 4.2.2). The hsCRP and LDL-C cut-off levels for the secondary analysis were chosen on the basis of results from an hypothesis-generating analysis[61] from an earlier study (the AFCAPS/TexCAPS [Air Force/ Texas Coronary Atherosclerosis Prevention Study][62]).[6,60] All efficacy analyses were conducted in the intent-to-treat population.[15] A total of 89 890 patients were screened for enrollment into the JUPITER trial, of which 72 000 were ineligible for inclusion (i.e. 5 patients needed to be screened to identify one eligible patient).[15] The most common reasons for exclusion were LDL-C levels 3.4 mmol/L (130 mg/dL) [37 611 patients] or hsCRP levels <2.0 mg/L (25 993 patients).[15]
4.1 Primary Analysis
The baseline characteristics of patients in the JUPITER trial did not appear to differ between treatment arms.[15] The median age of patients was 66.0 years, 38.2% of patients were women, and 25.2% were black or Hispanic.[15] There was a high percentage of patients with risk factors for CHD, with 58% having hypertension,[16] 41% having metabolic syndrome,[15] 23% having low HDL-C levels,[16] 16% being cigarette smokers,[15,16] and 12% having a family history of premature CHD;[15,16] approximately 17% of patients were receiving regular aspirin.[15] Based on the Framingham risk criteria, the estimated 10-year risk of developing CHD was 11.6% in the study patient population.[16] Median levels of LDL-C, HDL-C, and triglycerides at baseline were 2.8 mmol/L (108 mg/dL), 1.3 mmol/L (49 mg/dL), and 1.3 mmol/L (118 mg/dL), respectively, in both the rosuvastatin and placebo groups.[15] In the rosuvastatin group, the median baseline hsCRP level was 4.2 mg/L and, in the placebo group, it was 4.3 mg/L.[15]
4.1.1 Cardiovascular Events
Rosuvastatin significantly (p < 0.00001) reduced the occurrence of first major cardiovascular events in apparently healthy women and men with normal LDL-C levels and elevated hsCRP levels by almost one-half.[15] The rate per 100 person-years of first major cardiovascular events, as defined in figure 2, was 0.77 in the rosuvastatin group and 1.36 in the placebo group (primary endpoint; see figure 2 for actual event numbers).[15] The benefits of rosuvastatin over placebo for the prevention of first major cardiovascular events translated into a relative risk reduction of 44%[51] (hazard ratio [HR] 0.56; 95% confidence interval [CI]
Am J Cardiovasc Drugs 2010; 10 (6)
390
Carter
0.46, 0.69[15]), and a number of patients who needed to be treated (NNT) to prevent one first major cardiovascular event of 215,[51] 95,[15,51] 31,[15,51] and 25[15,51] after 1,[51] 2,[15,51] 4,[15,51] and 5[15,51] years of rosuvastatin treatment, respectively; the 4-year absolute risk rates were projected over an average 5-year treatment period to obtain the 5-year NNT value.[15,51] When each component of the primary endpoint was analyzed separately, a significant difference was seen between the rosuvastatin and placebo groups in the incidence of nonfatal MI (rate per 100 person-years 0.12 vs 0.33; p < 0.00001; HR 0.35; 95% CI 0.22, 0.58),[15,16] nonfatal stroke (rate per 100 person-years 0.16 vs 0.31; p = 0.003; HR 0.52; 95% CI 0.33, 0.80),[15,16] and arterial revascularization procedures (rate per 100 person-years 0.38 vs 0.71; p < 0.0001; HR 0.54; 95% CI 0.41, 0.72).[15,16] However, there was no significant between-group difference for the endpoints of hospitalization for unstable angina (rate per 100 person-years 0.09 vs 0.14 in the placebo group)[15] or cardiovascular deaths (rate per 100 person-years 0.19 vs 0.24).[16] See figure 2 for actual event numbers. Although the between-group difference in the incidence of cardiovascular deaths was not significant,[16] a between-group difference in favor of rosuvastatin was demonstrated for the incidence of deaths from any cause (198 vs 247 events; rate per 100 person-years 1.00 vs 1.25; p = 0.02; HR 0.80, 95% CI 0.67,
300 250 200 150 100 ** 50 * 0
re va A sc rte ul ria ar l iz at C io Vn re la te d de at hs N on fa ta ls tro ke al M I fo Ho ru s pi ns ta ta liz bl a e tio an n gi na ev en ts on fa t
ROS PL
***
***
0.97).[15] The incidence of noncardiovascular deaths was not reported. As well as reducing the incidence of nonfatal MI and of nonfatal stroke, rosuvastatin was also associated with a significant (p 0.002) reduction in the overall incidence of fatal or nonfatal MI (31 vs 68 events; rate per 100 person-years 0.17 vs 0.37; HR 0.46; 95% CI 0.30, 0.70)[15] and the overall incidence of fatal or nonfatal strokes (33 vs 64 events; rate per 100 personyears 0.18 vs 0.34; HR 0.52; 95% CI 0.34, 0.79)[15,53] relative to placebo. The between-group difference in the incidence of stroke was primarily accounted for by the difference in the incidence of ischemic stroke between the two groups (23 vs 47 events; rate per 100 person-years 0.12 vs 0.25; p = 0.004; HR 0.49; 95% CI 0.30, 0.81), with no significant between-group differences being demonstrated for the incidence of hemorrhagic stroke or transient ischemic attacks.[53] Rosuvastatin remained significantly more effective than placebo when primary endpoint results were stratified according to various baseline factors, including age, sex, race, and geographic region.[15] Moreover, a between-group difference in favor of rosuvastatin was demonstrated in all patient subgroups, regardless of whether they were at a low or high baseline risk of cardiovascular events.[15] For example, rosuvastatin was more effective than placebo in patients who did or did not smoke, in those with a body mass index (BMI) of <25.0, 25.029.9, or 30.0 kg/m2, in those with or without a history of hypertension or metabolic syndrome, and in those with or without a family history of CHD.[15] Furthermore, a betweengroup difference in favor of rosuvastatin was observed in patients with a Framingham risk score of 10% and in those with a score of >10%, and was also noted in patients who had at least one NCEP ATP III risk factor at baseline as well as in those who had none.[15] Moreover, relative to placebo, rosuvastatin significantly reduced the incidence of first major cardiovascular events occurring in patients who had no risk factors for CVD other than increased age and an elevated hsCRP level.[15] Results of analyses[54-59] in which primary endpoint results were stratified according to some of these (or other) key baseline factors are discussed further in section 4.2.2.
4.1.2 Thromboembolic Events
No. of events
al C V
Fig. 2. Efficacy of rosuvastatin (ROS) in preventing major cardiovascular (CV) events in apparently healthy women or men with normal low-density lipoprotein cholesterol levels, and elevated high-sensitivity C-reactive protein levels. Results of an interim analysis at a median follow-up of 1.9 years of the large, double-blind, multinational JUPITER trial in which patients (pts) were randomized to receive ROS 20 mg (n = 8901) or placebo (PL; n = 8901) once daily.[15,16] A major CV event was defined as a nonfatal myocardial infarction (MI), nonfatal stroke, hospitalization for unstable angina, an arterial revascularization procedure, or death due to a CV cause. Analyses were in the intent-to-treat population. * p = 0.003, ** p < 0.0001, *** p < 0.00001 vs PL.
2010 Adis Data Information BV. All rights reserved.
To t
Rosuvastatin also appeared to be effective in reducing the incidence of venous thromboembolism (i.e. pulmonary embolism or deep-vein thrombosis), with 34 events occurring in the rosuvastatin group versus 60 events in the placebo group (rate per 100 person-years 0.18 vs 0.32; p = 0.007; HR 0.57; 95% CI 0.37, 0.86).[52] A significant difference was also seen between rosuvastatin and placebo recipients for the combined incidence
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
391
of the primary composite endpoint and venous thromboembolism (173 vs 305 events; rate per 100 person-years 0.93 vs 1.66; p < 0.001; HR 0.56; 95% CI 0.47, 0.68).[52]
4.2 Secondary Analyses
4.2.1 Stratification According to On-Treatment Laboratory Measures
an LDL-C level <1.8 mmol/L (<70 mg/dL) had a 79% reduction in the risk (p = 0.037; HRfully adjusted 0.21; 95% CI 0.09, 0.51).[60] There was no relationship between on-treatment HDL-C or apoA1 levels and the incidence of first major cardiovascular events.[59]
4.2.2 Stratification According to Baseline Factors hsCRP, LDL-C, HDL-C, and Apolipoprotein A1 Levels
Rosuvastatin was associated with significant reductions in hsCRP and LDL-C levels (section 2.2).[60] However, it appeared that rosuvastatin recipients who achieved an LDL-C level of <1.8 mmol/L (<70 mg/dL) [n = 5606] at the 1-year followup may have had lower LDL-C levels at baseline than those who did not achieve this goal (n = 2110) [2.7 vs 2.9 mmol/L (104 vs 112 mg/dL); statistical analyses not available].[60] Similarly, it appeared that patients who achieved an hsCRP level of <2 mg/L (n = 3411) at the 1-year follow-up may have had lower hsCRP levels at baseline than those who did not achieve this goal (n = 4305) [3.2 vs 5.4 mg/L; statistical analyses not available].[60] A number of other potential confounding factors were also observed between the various groups and, thus, results were adjusted to account for these differences (table I).[60] Stratification of primary endpoint results according to the hsCRP and LDL-C levels achieved after 1 year of rosuvastatin therapy demonstrated that rosuvastatin-related reductions in these laboratory measures were associated with a favorable clinical response, which was not entirely explained by reductions in LDL-C levels alone.[60] For example, recipients of rosuvastatin who achieved an hsCRP level <2 mg/L (with or without a reduction in LDL-C levels <1.8 mmol/L [<70 mg/dL]) had a 62% reduction in the risk of a first major cardiovascular event occurring relative to recipients of placebo (p = 0.007; age-adjusted HR [HRage] 0.38; 95% CI 0.26, 0.56) and those who achieved an LDL-C level <1.8 mmol/L (<70 mg/dL) [with or without a reduction in hsCRP levels <2 mg/L] had a 55% reduction in the risk (p = 0.001; HRage 0.45; 95% CI 0.34, 0.60) [table I].[60] Moreover, although hsCRP and LDL-C level reductions were only weakly correlated in individual patients (Spearman correlation coefficient [r] = 0.10), rosuvastatin recipients with an LDL-C level <1.8 mmol/L (<70 mg/dL) and an hsCRP level of <2 mg/L, or, even more so, <1 mg/L had the lowest risk of a first major cardiovascular event occurring relative to the other subgroups (table I).[60] In terms of relative risk reduction, rosuvastatin recipients achieving an hsCRP level <2 mg/L and an LDL-C level <1.8 mmol/L (<70 mg/dL) had a 65% reduction in the risk of a first major cardiovascular event occurring relative to placebo recipients (p = 0.033; fully-adjusted HR [HRfully adjusted] 0.35; 95% CI 0.23, 0.54), and those achieving an hsCRP level <1 mg/L and
2010 Adis Data Information BV. All rights reserved.
In general, the risk of a first major cardiovascular event occurring in the JUPITER trial increased with increasing baseline hsCRP level.[58] In men, for every increase of one in the log-transformed hsCRP level, the risk of a primary endpoint event occurring increased by 1.3-fold (p = 0.002). Although results of this same analysis for the primary endpoint in women were not significant, similar findings to those observed in men were demonstrated for other efficacy endpoints. Because the rosuvastatin-associated relative risk reduction was similar across the hsCRP tertiles in men receiving rosuvastatin, the greatest reduction in the risk of a major cardiovascular event occurring in men was observed in those with hsCRP levels in the highest tertile at baseline (i.e. >5.4 mg/L). Although the relationship between baseline hsCRP levels and primary endpoint events was less clear in women for the tertile analysis, a significant relationship was seen for other endpoints.[58] Baseline HDL-C or apoA1 levels were not predictive of residual cardiovascular risk in rosuvastatin recipients.[59] In contrast to the placebo arm, in which the number of primary endpoint events occurring decreased with increasing HDL-C or apoA1 quartile, there was no relationship between baseline levels of HDL-C or apoA1 and the number of first cardiovascular events occurring in the rosuvastatin arm.[59]
Fasting Glucose Levels
Although there was a higher incidence of physician-reported diabetes in rosuvastatin recipients than in placebo recipients (section 5), the efficacy of rosuvastatin did not appear to be affected by fasting glucose levels, with the number of primary endpoint events being significantly lower in the rosuvastatin versus placebo groups in patients with impaired fasting glucose levels at baseline (n = 5504) [p = 0.037; HR 0.69; 95% CI 0.49, 0.98] as well as in those with normal fasting glucose levels at baseline (n = 12 170) [p < 0.001; HR 0.51; 95% CI 0.40, 0.67];[56] quantitative data are not available for this analysis.
Renal Dysfunction
Regardless of treatment group, patients with moderate chronic kidney disease (defined as an estimated glomerular filtration rate [eGFR] of <60 mL/min/1.73 m2) [n = 3267] were at a significantly
Am J Cardiovasc Drugs 2010; 10 (6)
392
Carter
Table I. Efficacy of rosuvastatin (ROS) in preventing the occurrence of first major cardiovascular (CV) events in apparently healthy women or men with normal low-density lipoprotein cholesterol (LDL-C) levelsa and elevated high-sensitivity C-reactive protein (hsCRP) levelsb in the JUPITER trial.[60] Incidence of the first occurrence of nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina, arterial revascularization procedures, and mortality due to a CV event over a median follow-up period of 1.9 years (maximum of 5 years) [primary endpoint] when stratified according to the hsCRP and LDL-C levels obtained after 1 year of treatment with ROS 20 mg or placebo (PL) once daily. Analyses are in the intent-to-treat population Pt group PL ROS hsCRP <2 mg/L hsCRP 2 mg/L LDL-C <1.8 mmol/L
d
No. of pts in subgroup 7832
No. of events 189
Incidence rate (per 100 person-y) 1.11
HRage adjusted (95% CI)c 1.00 0.38 (0.26, 0.56)* 0.69 (0.53, 0.91)* 0.45 (0.34, 0.60)** 0.89 (0.63, 1.25) 0.35 (0.23, 0.54)e 0.54 (0.27, 1.10) 0.55 (0.39, 0.77)e 1.06 (0.72, 1.55) 0.21 (0.09, 0.52) 0.50 (0.38, 0.67)
e e
HRfully adjusted (95% CI)c 1.00 0.36 (0.24, 0.54)e 0.68 (0.51, 0.89)e 0.45 (0.33, 0.59)e 0.85 (0.60, 1.21) 0.35 (0.23, 0.54)-0.42 (0.18, 0.94)e 0.53 (0.38, 0.74)e 1.06 (0.72, 1.55) 0.21 (0.09, 0.51)0.49 (0.37, 0.66)e 0.46 (0.11, 1.85) 0.89 (0.62, 1.28) 0.59 (0.46, 0.75)0.64 (0.49, 0.84)--
3411 4305 5606 2110 2685 726 2921 1384
d d
31 72 64 39 23 8 41 31 5 59 3 36 98 80
0.42 0.77 0.51 0.91 0.38 0.54 0.62 1.11 0.24 0.56 0.64 0.95 0.67 0.74
LDL-C 1.8 mmol/Ld hsCRP <2 mg/L and LDL-C <1.8 mmol/Ld hsCRP <2 mg/L and LDL-C 1.8 mmol/L hsCRP 2 mg/L and LDL-C <1.8 mmol/Ld hsCRP 2 mg/L and LDL-C 1.8 mmol/L
d
hsCRP <1 mg/L and LDL-C <1.8 mmol/LL hsCRP 1 mg/L and LDL-C <1.8 mmol/L
d
944 4662 236 1874 6772 5031
d
hsCRP <1 mg/L and LDL-C 1.8 mmol/Ld hsCRP 1 mg/L and LDL-C 1.8 mmol/Ld hsCRP 1 mg/L and/or LDL-C 1.8 mmol/Ld hsCRP 2 mg/L and/or LDL-C 1.8 mmol/L
0.65 (0.21, 2.03) 0.91 (0.64, 1.30) 0.61 (0.48, 0.77)e 0.67 (0.52, 0.87)
e
a The median LDL-C level at baseline was 2.8 mmol/L (108 mg/dL). b The median hsCRP level at baseline was 4.2 mg/L in the ROS group and 4.3 mg/L in the PL group. c Hazard ratios (HR) were fully adjusted for age (HRage adjusted) or for age, sex, blood pressure, body mass index, smoking status, parental history of premature coronary heart disease, and baseline LDL-C, hsCRP, and HDL-C levels (HRfully adjusted). d An LDL-C level of <1.8 mmol/L is equivalent to a level of <70 mg/dL. e p-Value not reported.[60] HDL-C = high-density lipoprotein cholesterol; pt = patient. fully-adjusted analysis.
*
p = 0.007,
**
p = 0.001 vs PL in the age-adjusted analysis; - p = 0.037, -- p = 0.033 vs PL in the
(p = 0.0002) higher risk of first major cardiovascular events than those with normal kidney function (defined as an eGFR 60 mL/min/1.73 m2) [n = 14 528], as demonstrated by a significantly higher number of primary endpoint events reported in patients with moderate chronic kidney disease versus those with normal renal function (incidence rate per 100 person-years 1.51 vs 0.95; HR 1.54; 95% CI 1.23, 1.92).[57] All other baseline characteristics differed significantly (p 0.03) between patients with moderate chronic kidney function and those with normal kidney function, but there were no differences in the baseline characteristics of patients with moderate chronic kidney function who received rosuvastatin and those who received placebo.[57] The efficacy of rosuvastatin was not altered by the presence of renal dysfunction.[57] For example, rosuvastatin was associated with a significantly lower number of primary endpoint events than
2010 Adis Data Information BV. All rights reserved.
placebo in both the subgroup of patients with moderate chronic kidney disease (rate per 100 person-years 1.08 vs 1.95; p = 0.002; HR 0.55; 95% CI 0.38, 0.82) and in the subgroup with normal renal function (incidence rate per 100 person-years 0.69 vs 1.21; p < 0.001; HR 0.57; 95% CI 0.45, 0.72). This translated into a 5-year NNT of 14 in the subgroup of patients with moderate chronic kidney disease and 35 in the subgroup with normal kidney function.[57]
Sex of Patient
Aside from the proportion of women and men receiving aspirin (16.4% vs 16.8%) and the baseline triglyceride levels (both 1.3 mmol/L [118 mg/dL]), all other baseline characteristics differed significantly (p 0.02) between women (n = 6801) and men (n = 11 001).[55] For example, women were older than men (median age of 68 vs 63 years), smoked less (7.6% vs
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
393
21.0%), were more likely to have metabolic syndrome (46.7% vs 38.7%), and had higher hsCRP (median of 4.6 vs 4.1 mg/L) and LDL-C (2.82 vs 2.80 mmol/L [109 vs 108 mg/dL]) levels.[55] Rosuvastatin effectively reduced the number of first major cardiovascular events occurring in both women and men.[55] Although the primary endpoint incidence rates in rosuvastatin or placebo recipients appeared to be lower in women (0.56 vs 1.04 per 100 person-years; p = 0.002) than in men (0.88 vs 1.54 per 100 person-years; p < 0.0001), the relative risk reduction was similar in both women (HR 0.54; 95% CI 0.37, 0.80) and men (HR 0.58; 95% CI 0.45, 0.73). The benefit of rosuvastatin over placebo in preventing one first major cardiovascular event translated into a 5-year NNT of 36 in women and 22 in men.[55]
Age of Patient
Relative to younger patients (aged 5069 years; n = 12 107), elderly patients (aged 7097 years; n = 5695) appeared more likely to have hypertension (5354% vs 66%) or a Framingham risk score of >10 (41% vs 69%), but less likely to be obese (i.e. BMI of 30 kg/m2) [40% vs 3233%] or to be smokers (19% vs 89%) [statistical analyses not available].[54] Most other baseline characteristics were similar between the two groups, although it appeared that more elderly than younger patients were women (5152% vs 32%).[54] Within these subgroups, there did not appear to be any between-group differences in the baseline characteristics of patients who received rosuvastatin and those who received placebo.[54] Patient age did not appear to affect the efficacy of rosuvastatin in reducing the occurrence of first major cardiovascular events, with the number of primary endpoint events being significantly (p < 0.001) lower in both elderly (75 vs 119 events; rate per 100 person-years 1.22 vs 1.99; HR 0.61; 95% CI 0.46, 0.82) and younger (67 vs 132 events; rate per 100 person-years 0.54 vs 1.06; HR 0.51; 95% CI 0.38, 0.69) rosuvastatin recipients than in placebo recipients.[54] The absolute treatment effect was 0.77 per 100 person-years in those aged 70 years (95% CI 0.32, 1.22) and 0.52 per 100 person-years in those aged <70 years (95% CI 0.29, 0.74), and this translated into a 4-year NNT of 24 and 36,[54] and a 5-year NNT of 19 and 29.[51] 5. Tolerability The tolerability profile of rosuvastatin has been well described previously.[7,17,18] This section focuses on the tolerability profile of rosuvastatin in apparently healthy women and men with normal LDL-C levels and elevated hsCRP levels, as observed in the JUPITER trial.[15] Patients in this trial received rosuvastatin 20 mg (n = 8901) or placebo (n = 8901) once daily.[15] Results are from an interim analysis conducted at a median duration of 1.9
2010 Adis Data Information BV. All rights reserved.
years (maximum duration of 5 years)[15] [see section 4 for further study design details and efficacy results]. Rosuvastatin was generally well tolerated in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels, with serious adverse events occurring at a similar frequency in the rosuvastatin versus placebo arms (15.2% vs 15.5%).[15] Study discontinuations due to adverse events occurred in 6.6% of rosuvastatin recipients and 6.2% of placebo recipients, with myalgia being the most common cause.[16] The most frequently reported treatment-related adverse events associated with rosuvastatin were myalgia, arthralgia, constipation, and nausea (figure 3; statistical analyses not available for these results).[16] The nature of these treatment-related adverse events was similar to those in a pooled safety analysis of clinical trial data (n = 5394; rosuvastatin 540 mg/day) presented in the manufacturers US prescribing information[16] and a pooled safety analysis[63] of an integrated clinical trial database of 33 trials (n = 16 876; rosuvastatin 540 mg/day) discussed in a previous review.[7] Moreover, the incidences of rosuvastatin-related myalgia, nausea, and constipation reported in the JUPITER trial (figure 3) were similar to the incidences (myalgia [6.3%], constipation [4.7%], and nausea [6.3%]) reported in patients receiving rosuvastatin 20 mg (n = 64) in the placebo-controlled trials (n = 744; rosuvastatin dose 540 mg) included in the pooled safety analysis reported in the manufacturers prescribing information.[16] Arthralgia was not among the most commonly reported rosuvastatin-related adverse events in this pooled analysis.[16] In general, the incidence of monitored adverse events (figure 4) and the levels of laboratory measurements at study endpoint were
10 9 8 7 Patients (%) 6 5 4 3 2 1 0 Myalgia Arthralgia Constipation Nausea
ROS PL
Fig. 3. Tolerability of rosuvastatin (ROS) in apparently healthy women or men with normal low-density lipoprotein cholesterol levels and elevated highsensitivity C-reactive protein levels. Incidence of treatment-related adverse events occurring in patients receiving ROS 20 mg (n = 8901) or placebo (PL; n = 8901) once daily in the pivotal JUPITER trial.[16] Results are from an interim analysis at a median follow-up duration of 1.9 years.
Am J Cardiovasc Drugs 2010; 10 (6)
394
Carter
similar in the rosuvastatin and placebo groups.[15] However, the median glomerular filtration rate at 12 months (66.8 vs 66.6 mL/min/1.73 m3; p = 0.02) and the median glycosylated hemoglobin level at 24 months (5.9% vs 5.8%; p = 0.001) were significantly higher in the rosuvastatin versus placebo groups.[15] Increases in glycated hemoglobin and fasting serum glucose levels have been reported previously with statins, including rosuvastatin.[16] Although there was no significant between-group difference in the median fasting glucose level at 24 months (98 mg/dL [5.4 mmol/L] in both groups) or the proportion of patients with glycosuria at 12 months (36% vs 32%) in the JUPITER trial, newly diagnosed (by a physician) diabetes was reported in a significantly higher proportion of patients in the rosuvastatin arm than in the placebo arm (3.0% vs 2.4% of patients; p = 0.01).[15] Statins, including rosuvastatin, have been associated with rare cases of myopathy and rhabdomyolysis with acute renal failure secondary to myoglobinuria.[16] The risk of such adverse events occurring is highest at a rosuvastatin dose of 40 mg, but they may also occur at lower doses.[16] The risk of developing myopathy with rosuvastatin may also be increased by coadministration with various other drugs (e.g. fibric acid derivatives or niacin), and a reduction in the dose of rosuvastatin is recommended for some combinations (section 2.5). In addition, caution should be exercised when using rosuvastatin in patients with an increased risk of developing skeletal muscle-
25
ROS PL
20
15
10
5 * 0
rd er M sy us m cu pt la om r R s# en al di so rd N er ew D x ca nc er N ew D x D M ng er is o ee di so rd ca nc e r
Fig. 4. Tolerability of rosuvastatin (ROS) in apparently healthy women or men with normal low-density lipoprotein cholesterol levels and elevated highsensitivity C-reactive protein levels. Incidence of monitored adverse events occurring in patients receiving ROS 20 mg (n = 8901) or placebo (PL; n = 8901) once daily in the pivotal JUPITER trial.[15] Results are from an interim analysis at a median follow-up duration of 1.9 years. DM = diabetes mellitus; Dx = diagnosis; GI = gastrointestinal; # = muscular symptoms included muscular weakness, stiffness, or pain. * p = 0.01 vs ROS.
2010 Adis Data Information BV. All rights reserved.
related adverse events, such as patients aged 65 years, or those with uncontrolled hypothyroidism or renal impairment.[16] Rosuvastatin should be discontinued if the patient develops markedly elevated creatinine kinase levels or myopathy (either confirmed or suspected), and the drug withheld if the patient develops any acute, serious condition that may be suggestive of myopathy or that may predispose them to developing renal failure secondary to rhabdomyolysis (e.g. dehydration, hypotension, major surgery, sepsis, trauma, uncontrolled seizures, or a severe electrolyte, endocrine, or metabolic disorder).[16] In the JUPITER trial, ten episodes of myopathy occurred in 8901 patients in the rosuvastatin group (0.1%) and nine episodes occurred in 8901 patients in the placebo group (0.1%).[15] One episode of rhabdomyolysis was reported in a rosuvastatin recipient after the trial had been closed; this event was nonfatal and occurred in an elderly patient (aged 90 years) with febrile influenza, pneumonia, and trauma-induced myopathy,[15] and a history of moderate chronic kidney disease.[57] Elevations in transaminase levels have also been reported with statins, with 1.1% of rosuvastatin recipients and 0.5% of placebo recipients having a serum transaminase level of >3 the ULN in a pooled analysis of placebo-controlled trials reported in the manufacturers prescribing information.[16] Most transaminase elevations are transient and resolve or improve with continued treatment or a brief drug-free period.[16] However, rare cases of jaundice have been reported.[16] Because of this, serum transaminase levels should be measured before initiation of rosuvastatin, 12 weeks after initiation of rosuvastatin or a dose adjustment, and periodically thereafter.[16] If ALT or AST levels remain >3 the ULN, the dose of rosuvastatin should be decreased or the drug discontinued.[16] Rosuvastatin should be used with caution in patients with a history of chronic liver disease or excess alcohol use, and is contraindicated in those with active liver disease (section 3.3).[16] In the JUPITER trial, elevation of ALT levels to >3 the ULN on consecutive visits occurred in 0.3% of patients (23 events in 8901 patients) in the rosuvastatin arm and 0.2% (17 events in 8901 patients) in the placebo arm.[15] Although atorvastatin (another statin) was associated with a significantly higher incidence of hemorrhagic strokes than placebo in a previous clinical study,[64] the incidence of hemorrhagic strokes in the JUPITER trial was low and similar in both the rosuvastatin and placebo treatment arms (6 [0.07%] vs 9 [0.10%] events in 8901 patients).[15] Rosuvastatin demonstrated a similar tolerability profile in patients with moderate chronic kidney disease versus those with normal renal function.[57] However, the number of patients with newly diagnosed diabetes was significantly higher in recipients of rosuvastatin than placebo in the group of patients with normal
Am J Cardiovasc Drugs 2010; 10 (6)
Patients (%)
Id
Bl
di
ic
ep at
ea t
fro
Rosuvastatin: A Review
395
renal dysfunction (216 vs 164 events; p = 0.01) but not in those with moderate chronic kidney disease (54 vs 52 events), as was the incidence of newly diagnosed renal disorders (388 vs 339 events [p = 0.05] and 146 vs 141 events).[57] The one case of rhabdomyolysis that occurred during the trial was in a rosuvastatin recipient with moderate chronic kidney disease.[57] In general, sex did not appear to affect the tolerability profile of rosuvastatin.[55] However, the incidence of newly diagnosed diabetes was significantly higher in women receiving rosuvastatin than in those receiving placebo (108 vs 71 events; p = 0.008), whereas there was no significant between-group difference in the incidence of newly diagnosed diabetes in men (162 vs 145 events) [p-value for heterogeneity of diabetes by sex = 0.16].[55] Of interest, although previous reports suggested the possibility of women having an increased risk of cancer-related deaths with statin treatment over placebo (reviewed by Mora et al.[55]), no such finding was observed in the JUPITER trial, with death related to cancer being reported in 0.2% of women in both the rosuvastatin and placebo groups, and in 0.2% and 0.3% of men receiving rosuvastatin or placebo (p = 0.03).[55] In the JUPITER trial, elderly patients (aged 7097 years) appeared to have a higher incidence of monitored adverse events and serious adverse events than younger patients (aged 5069 years), regardless of treatment arm (no statistical comparison available).[54] However, no statistically significant differences were demonstrated between rosuvastatin and placebo recipients with regard to the incidence of the majority of monitored adverse events in either the elderly or younger patient groups.[54] The only between-group difference identified was in the incidence of bleeding events, which occurred at a significantly lower rate in rosuvastatin than placebo recipients in the younger age group (rate per 100-person years 1.03 vs 1.32; HR 0.78; 95% CI 0.62, 0.98).[54] 6. Dosage and Administration In the US, rosuvastatin is approved as an adjunctive therapy to a healthy diet (i.e. a diet low in saturated fat and cholesterol) in adult patients with primary hyperlipidemia, mixed dyslipidemia, hypertriglyceridemia, or primary dysbetalipoproteinemia (hyperlipoproteinemia type III), and in combination with other lipidlowering drugs (or alone if no other treatments are available) in adults with homozygous familial hypercholesterolemia.[16] It is also approved for use in pediatric patients (aged 1017 years) with heterozygous familial hypercholesterolemia, and to slow the progression of atherosclerosis in adults.[16] More recently, rosuvastatin has also been approved for use in the primary prevention of CVD (i.e. MI, stroke, or arterial revascularization procedures) in patients with no clinical evidence of CHD
2010 Adis Data Information BV. All rights reserved.
who are at increased risk of developing CVD based on their age (60 years for women and 50 years for men), an hsCRP level of 2 mg/L, and the presence of 1 other risk factor (e.g. hypertension, low HDL-C level, smoking, or a family history of premature CHD).[16] In general, the recommended dosage of rosuvastatin for the approved indications is 540 mg once daily, with the usual starting dosage being 1020 mg once daily.[16] In the JUPITER trial, the benefit of rosuvastatin over placebo in reducing the incidence of major cardiovascular events in apparently healthy women or men with normal LDL-C levels and elevated hsCRP levels was demonstrated at a rosuvastatin dosage of 20 mg once daily (section 4). According to the manufacturers US prescribing information, rosuvastatin should be started at a lower dose and then titrated according to response and individual targets.[16] Where relevant, only patients who have not achieved the target LDL-C level with rosuvastatin 20 mg should receive rosuvastatin 40 mg.[16] Rosuvastatin can be administered at any time of the day, without regard for food.[16] In the US, rosuvastatin dose reductions (or restrictions) are recommended in patients receiving concomitant fenofibrate or niacin (section 2.5), and in those receiving concomitant gemfibrozil (if the combination is unavoidable), cyclosporine, atazanavir/ritonavir, or lopinavir/ritonavir (section 3.4).[16] Dose reductions are also recommended in Asian patients or patients with severe renal impairment who are not receiving hemodialysis (section 3.3).[16] Local prescribing information should be consulted for further information regarding contraindications, warnings, precautions, dose adjustments, and use in special populations. 7. Place in the Prevention of Cardiovascular Disease in Apparently Healthy Women or Men with Normal LDL-C Levels and Elevated hsCRP Levels CVD is the leading cause of death in the US, and is associated with a large economic burden.[1] In the US in 2010, the total direct and indirect costs incurred by this disease will reach an estimated $US503.2 billion.[1] Furthermore, it has been estimated that CVD (including CHD and diabetes) will cost US society up to $US9.5 trillion over the next 30 years (2008 estimate).[65] Prevention of CVD involves the detection and treatment of modifiable CVD risk factors.[2] Risk interventions currently recommended by US guidelines include control of blood pressure and blood lipids (via lifestyle modifications and/or pharmacologic therapy); management of medical conditions, such as diabetes and chronic atrial fibrillation; administration of aspirin to patients at a higher risk of CHD than others, particularly those with a 10-year Framingham risk of 10%; and a
Am J Cardiovasc Drugs 2010; 10 (6)
396
Carter
variety of lifestyle modifications, including complete cessation of smoking, adoption of a healthy eating pattern, bodyweight management, and regular physical exercise.[2] According to NCEP, a 2030% reduction in LDL-C levels may be achieved by losing 10 pounds (if overweight) and changing to a more suitable diet (i.e. one high in soluble fiber and plant sterols/ stanols, but low in saturated fat and cholesterol).[66] Assuming a 100% efficacy, if all patients adopted recommended healthy lifestyle practices and received all the risk interventions for which they were eligible, an estimated two-thirds of MIs and one-third of strokes would be prevented in the US each year.[65] However, the cost of utilizing such strategies would increase the direct medical cost associated with CVD by $US7.6 trillion over a 30-year period (2008 costs).[65] One way in which the economic burden associated with CVD may be reduced is by improvement of the Framingham risk model, with the aim of reclassifying a proportion of intermediaterisk patients into the low- or high-risk categories.[3] If additional CVD risk factors were identified and added into the model, then it is possible that preventative treatment may be reserved for those who are likely to benefit from it, thereby allowing the benefits of screening to be maximized and any associated harms (e.g. adverse effects associated with drugs, false-positive results, unnecessary invasive diagnostic procedures) to be minimized.[3] HsCRP is a sensitive (but nonspecific) inflammatory biomarker that is independently associated with incident CHD events,[67] and may be of use in assessing CVD risk.[67,68] Elevated CRP levels are associated with CVD risk factors, such as obesity, smoking, and inactivity, and various longitudinal studies have demonstrated a reduction in CRP levels of up to 41% after introduction of long-term (at least 6 months) exercise training (reviewed by Plaisance and Grandjean[69]). The inflammatory hypothesis of atherothrombosis has gathered much evidence over the past two decades, and it now appears that inflammation plays a fundamental role in the mediation of atherothrombosis at all stages of the disease.[70,71] Of the various inflammatory markers that were considered by the Centers for Disease Control and Prevention (CDC) and the American Heart Association (AHA) as potentially useful predictors of CVD risk, hsCRP was the favored option because of its stability, and the availability, precision, accuracy, and standardization of the assay.[71] Rosuvastatin is an HMG-CoA reductase inhibitor (statin) that was shown to lower hsCRP levels (and improve lipid levels) in numerous clinical trials conducted in patients with dyslipidemia, including those at high-risk of developing CVD and those with established CVD (sections 1 and 2.2). Where investigated, these hsCRP level reductions were associated with clinical benefit (sections 1 and 2.2). The pivotal JUPITER trial was de 2010 Adis Data Information BV. All rights reserved.
signed to further explore the relationship between rosuvastatinassociated reductions in hsCRP levels and the prevention of CVD.[15] Patients eligible for this trial were apparently healthy individuals with normal LDL-C (<3.4 mmol/L [<130 mg/dL]) and triglyceride (<5.65 mmol/L [<500 mg/dL]) levels, and elevated hsCRP levels (2.0 mg/L) [section 4]. All patients in the JUPITER trial had baseline LDL-C levels that fell below the recommended NCEP ATP III goal of <3.4 mmol/L (<130 mg/dL) and, thus, would not normally have been eligible for treatment with a statin.[4] Nonetheless, rosuvastatin significantly reduced the incidence of first major cardiovascular events occurring in the trial by almost one-half relative to placebo (primary endpoint; section 4.1.1 and figure 2). The incidences of MI (nonfatal or nonfatal plus fatal), stroke (nonfatal or nonfatal plus fatal; primarily ischemic stroke), arterial revascularization, and death from any cause were also significantly decreased with rosuvastatin versus placebo (section 4.1.1), as was the incidence of the nonatherothrombotic endpoint of venous thromboembolism (section 4.1.2). No statistical between-group difference was demonstrated in the incidences of cardiovascular death or hospitalization for unstable angina (section 4.1.1). The beneficial effects of rosuvastatin were observed in all patient subgroups (sections 4.1.1 and 4.2), including those thought to be at low-risk of developing CVD, such as patients with elevated hsCRP levels but no other risk factors for CVD except for age (section 4.1.1). Furthermore, the 5-year NNT for the JUPITER primary endpoint (25) was similar to (or numerically smaller than) those observed in previous primary prevention trials of statins that predominantly enrolled men with dyslipidemia (4070) and in secondary prevention trials in high-risk patients (1533) [reviewed by Ridker et al.[51] and by Libby and Crea[72]]. In addition, the JUPITER 5-year NNT for the primary endpoint was numerically smaller than those previously published for other well established preventative therapies, including antihypertensive drugs (80160) and aspirin (>300).[51,72] Therefore, it is possible that a number of patient subgroups who would not normally be eligible for preventative therapy with statins may benefit from receiving such drugs, and that these benefits may be similar to those of other preventative therapies already considered to be effective.[51] However, caution should be exercised when comparing NNT values across different trials and for different drugs.[51] Although some of the observed between-group difference in the incidence of the primary endpoint in the JUPITER trial may have been attributable to further lowering of LDL-C levels to <1.8 mmol/L (<70 mg/dL), a between-group difference in favor of rosuvastatin was also observed in the patient groups that did not achieve an LDL-C level of <1.8 mmol/L (<70 mg/dL) but did
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
397
achieve an hsCRP level of <1 or <2 mg/L (section 4.2.1). Furthermore, the greatest reductions in the risk of first major cardiovascular events were seen in the groups of patients achieving both an LDL-C level of <1.8 mmol/L (<70 mg/dL) and an hsCRP level of <2 mg/L or, even more so, <1 mg/L. Of interest, a retrospective analysis of results from the placebo cohort in the JUPITER trial demonstrated that tracking of hsCRP levels was strong throughout the trial, indicating that hsCRP levels would most likely have remained elevated in the absence of rosuvastatin treatment.[73] Therefore, the beneficial effect of rosuvastatin in preventing CVD appears to be attributable to both its lipid-lowering and antiinflammatory effects.[60] When JUPITER inclusion criteria (i.e. hsCRP and LDL-C levels) were retrospectively applied to individuals participating in the 19992004 National Health and Nutrition Examination Survey (a nationwide survey thought to be representative of the general US population), it was demonstrated that 6.5 million women (aged 60 years) and men (aged 50 years) would have been eligible for inclusion in the trial.[68] Furthermore, although not all would have been eligible for the JUPITER trial, an estimated 10.0 million elderly patients (i.e. aged 60 years for women and 50 years for men) and 54.4 million patients aged 20 years would be newly eligible for statin therapy based on an hsCRP level of 2 mg/L,[68] assuming that these individuals would not otherwise have met criteria for statin therapy because of optimal lipid levels (i.e. lipid levels below recommended NCEP ATP III goals for drug therapy).[68] Moreover, it has been predicted through modelling that the addition of hsCRP levels to traditional CVD risk factors would result in the reclassification of 11% of intermediate-risk men into the high-risk category and, if appropriate preventative strategies were instigated, that this would prevent 47.8 CHD events per 1000 men aged 4079 years.[3] The use of hsCRP levels in the CVD risk stratification process shows much promise.[61] However, there is much debate about the appropriateness of adding this nontraditional risk factor to those that are already well established.[72,74] Current US guidelines do not recommend measuring hsCRP levels for the purpose of CVD risk stratification in asymptomatic patients with no history of CVD[3] or in the general population.[71] However, the CDC/AHA guidelines do support the use of hsCRP levels as an additional marker of CVD risk in specific populations of patients, particularly those who are determined to be at an intermediate risk of CVD disease when traditional risk factors are taken into account.[71] According to these guidelines, this latter recommendation would allow clinicians to reclassify intermediate-risk patients into high- or low-risk groups, thereby further clarifying whether the patient would or would not benefit from further investigations and/or instigation of preventative therapies.[71]
2010 Adis Data Information BV. All rights reserved.
Physicians may also find it useful to measure hsCRP levels in patients with metabolic syndrome.[75] Moreover, JUPITER study investigators indicate that hsCRP levels should be measured in conjunction with lipid levels in all postmenopausal women and in all male patients aged 50 years.[6] The instigation of rosuvastatin (or another statin) on the basis of elevated hsCRP levels is another area of controversy.[51] The CDC/AHA guidelines do not make risk intervention recommendations based on hsCRP levels, although these guidelines have not been updated since the JUPITER trial results became available.[71] However, according to the lead investigator for the JUPITER trial, high-dose statins, such as rosuvastatin, should be considered in postmenopausal women and men aged 50 years who are found on two occasions to have an hsCRP level >2 mg/L or any other traditional risk factor (e.g. an LDL-C level >4.1 mmol/L [>160 mg/dL] or a total cholesterol : HDL-C ratio of >6) for which a statin would be prescribed.[6] In patients of this demographic with an hsCRP level <2 mg/L, an LDL-C level <4.1 mmol/L (<160 mg/dL), no family history of premature atherosclerosis, and no personal history of CVD or diabetes, initiation of statin therapy was not thought to be cost effective and, hence, was not recommended.[6] However, concern exists around the design of the JUPITER trial, particularly with regard to the mechanism of benefit of rosuvastatin and whether CVD risk can be reduced solely through the inhibition of the inflammatory process.[72,76] To address these concerns and further assess the inflammatory hypothesis of atherothrombosis, a randomized, double-blind, placebo-controlled trial (CIRT [Cardiovascular Inflammation Reduction Trial]) is currently investigating the use of very low dose methotrexate versus placebo in the secondary prevention of major cardiovascular events in patients with known CVD and persistently elevated CRP levels despite usual cardiovascular treatments.[76] Methotrexate has previously been shown to reduce several inflammatory biomarkers without affecting other components of the atherothrombotic process.[76] Therefore, if the CIRT trial was to demonstrate a clear benefit of methotrexate over placebo, then the inflammatory hypothesis of atherothrombosis would gain further weight and a new approach to the prevention of CVD may potentially be identified.[76] Another point of concern related to the design of the JUPITER trial was the exclusion of patients with normal hsCRP levels,[77-79] meaning that it was not possible to establish whether the beneficial effects of rosuvastatin were confined to patients with elevated hsCRP levels or whether patients with normal hsCRP levels would also benefit from receiving the drug.[77] Such patients were not included the trial because previous studies had failed to demonstrate any benefit of statin treatment in this patient
Am J Cardiovasc Drugs 2010; 10 (6)
398
Carter
population.[15] Although it would be helpful to evaluate the efficacy of rosuvastatin in patients with elevated hsCRP versus those with normal hsCRP in order to further clarify the use of hsCRP levels in CVD risk assessment,[78] it is unlikely that such a study will be conducted as it is unlikely to be feasible in terms of statistical power and sample size.[15] However, recent results from a retrospective analysis[80] of the randomized, placebo-controlled, METEOR (Measuring Effects on intima media Thickness: an Evaluation Of Rosuvastatin) trial[81] demonstrated that rosuvastatin 40 mg once daily significantly reduced hsCRP levels in patients with normal baseline hsCRP levels (plus elevated LDL-C levels and modest carotid intima-media thickness) who were thought to be at low-risk of CVD, and that these reductions were independent of the rosuvastatin-associated LDL-C effects.[80] Therefore, it can be concluded that rosuvastatin is also effective in patients with normal hsCRP levels, and that rosuvastatin-associated reductions in hsCRP levels occur through an independent pathway and are unlikely to be a secondary result of LDL-C level reductions, as has previously been suggested.[80] Rosuvastatin was generally well tolerated in the JUPITER trial, with the majority of adverse events being mild to moderate in severity and similar to those observed in other populations of patients receiving rosuvastatin in clinical trials (section 5). Myalgia, arthralgia, constipation, and nausea were the most commonly reported treatment-related adverse events (figure 3). In general, the incidences of monitored adverse events (figure 4) and laboratory measurements at study endpoint were similar in the rosuvastatin and placebo groups. However, newly diagnosed diabetes (physician assessed) was reported in a significantly higher proportion of rosuvastatin than placebo recipients throughout the study (section 5). In addition, the median glomerular filtration rate at 12 months and the median glycosylated hemoglobin level at 24 months were significantly higher in the rosuvastatin than placebo groups. None of these endpoints were adjudicated by the endpoint committee.[15] Furthermore, no significant betweengroup difference was demonstrated in the systematic protocol specified measurements of fasting blood glucose and glycosuria.[15] However, increases in glycosylated hemoglobin and fasting serum glucose levels have previously been reported with statins (including rosuvastatin) in other patient populations.[16] In a recent meta-analysis of 13 randomized, placebocontrolled or standard-of-care statin trials (n = 91 140) that included data from the JUPITER trial, an additional 174 cases of incident diabetes were reported in statin versus placebo/ standard-of-care recipients and this translated into a 9% increase in the risk of diabetes in these patients during the 3- to 4-year treatment period.[82] In absolute terms, this amounted to
2010 Adis Data Information BV. All rights reserved.
one new case of diabetes per 255 patients receiving statin therapy for 4 years, or 12.23 cases per 1000 patient-years; the corresponding rate with standard-of-care treatment was 11.25 cases per 1000 patient-years.[82] Elderly patients appeared to be at particularly high risk of statin-associated dysglycemia, according to a meta-regression analyses of these pooled data.[82] Although this increased risk should be taken into account when considering the use of statins in patients at low risk for CVD or in those groups for which statin treatment has not been proven, patients in whom statins are indicated should continue to receive these drugs because of the clear benefits they have in preventing macrovascular disease.[82] However, it is recommended that elderly statin recipients are monitored for dysglycemia throughout the treatment period.[82] In conclusion, rosuvastatin is an HMG-CoA reductase inhibitor that has both lipid-lowering and anti-inflammatory effects. In the JUPITER trial, the drug was effective in preventing first major cardiovascular events in apparently healthy women (aged 60 years) or men (aged 50 years) with normal LDL-C levels and elevated hsCRP levels. It is not yet clear whether the mechanism of benefit of rosuvastatin is related to its lipidlowering properties, anti-inflammatory properties, or a mixture of both. Furthermore, administration of rosuvastatin based solely on elevated hsCRP levels remains controversial. However, regardless of these issues, rosuvastatin remains an important pharmacologic option in the prevention of CVD, and may potentially be of benefit in certain subgroups of patients in whom statins would not normally be indicated. Disclosure
The preparation of this review was not supported by any external funding. During the peer review process, the manufacturer of the agent under review was offered an opportunity to comment on this article. Changes resulting from comments received were made on the basis of scientific and editorial merit.
References
1. American Heart Association. Heart disease and stroke statistics: 2010 update at-a-glance [online]. Available from URL: http://www.americanheart.org/ downloadable/heart/1265665152970DS-3241%20HeartStrokeUpdate_2010. pdf [Accessed 2010 May 12] 2. Pearson TA, Blair SN, Daniels SR, et al. AHA guidelines for primary prevention of cardiovascular disease and stroke: 2002 update: consensus panel guide to comprehensive risk reduction for adult patients without coronary or other atherosclerotic vascular diseases. Circulation 2002 Jul 16; 106 (3): 388-91 3. U.S. Preventive Services Task Force. Using nontraditional risk factors in coronary heart disease risk assessment: U.S. preventive services task force recommendation statement. Ann Intern Med 2009 Oct 6; 151 (7): 474-82 4. National Cholesterol Education Program. Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III):
Am J Cardiovasc Drugs 2010; 10 (6)
Rosuvastatin: A Review
399
executive summary [online]. Available from URL: http://www.nhlbi.nih.gov/ guidelines/cholesterol/atp3xsum.pdf [Accessed 2010 May 12] 5. Khot UN, Khot MB, Bajzer CT, et al. Prevalence of conventional risk factors in patients with coronary heart disease. JAMA 2003 Aug 20; 290 (7): 898-904 6. Ridker PM. Moving toward new statin guidelines in a post-JUPITER world: principles to consider. Curr Atheroscler Rep 2009 Jul; 11 (4): 249-56 7. Keating GM, Robinson DM. Rosuvastatin: a review of its effect on atherosclerosis. Am J Cardiovasc Drug 2008; 8 (2): 127-46 8. Ridker PM, Rifai N, Pfeffer MA, et al. Long-term effects of pravastatin on plasma concentration of C-reactive protein. Circulation 1999 Jul 20; 100 (3): 230-5 9. Albert MA, Danielson E, Rifai N, et al. Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/CRP evaluation (PRINCE): a randomized trial and cohort study. JAMA 2001 Jul 4; 286 (1): 64-70 10. Ridker PM, Rifai N, Pfeffer MA, et al. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Circulation 1998 Sep 1; 98 (9): 839-44 11. Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005 Jan 6; 352 (1): 20-8 12. Morrow DA, de Lemos JA, Sabatine MS, et al. Clinical relevance of C-reactive protein during follow-up of patients with acute coronary syndromes in the Aggrastat-to-Zocor trial. Circulation 2006 Jul 25; 114 (4): 281-8 13. Ridker PM, Morrow DA, Rose LM, et al. Relative efficacy of atorvastatin 80 mg and pravastatin 40 mg in achieving the dual goals of low-density lipoprotein cholesterol <70 mg/dl and C-reactive protein <2 mg/l: an analysis of the PROVE-IT TIMI-22 trial. J Am Coll Cardiol 2005 May 17; 45 (10): 1644-8 14. Ridker PM, on behalf of the JUPITER study group. Rosuvastatin in the primary prevention of cardiovascular disease among patients with low levels of low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein: rationale and design of the JUPITER trial. Circulation 2003 Nov 11; 108 (19): 2292-7 15. Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008 Nov 20; 359 (21): 2195-207 16. AstraZeneca. Crestor (rosuvastatin calcium) tablets: highlights of the US prescribing information [online]. Available from URL: http://www.accessdata.fda. gov/drugsatfda_docs/label/2010/021366s016lbl.pdf [Accessed 2010 May 12] 17. Carswell CI, Plosker GL, Jarvis B. Rosuvastatin. Drugs 2002; 62 (14): 2075-85 18. Scott LJ, Curran MP, Figgitt DP. Rosuvastatin: a review of its use in the management of dyslipidemia. Am J Cardiovasc Drugs 2004; 4 (2): 117-38 19. Niemi M. Transporter pharmacogenetics and statin toxicity. Clin Pharmacol Ther 2010 Jan; 87 (1): 130-3 20. Tomlinson B, Hu M, Lee VWY, et al. ABCG2 polymorphism is associated with the low-density lipoprotein cholesterol response to rosuvastatin. Clin Pharmacol Ther 2010; 87: 558-62 21. Hu M, Lui SSH, Mak VWL, et al. Pharmacogenetic analysis of lipid responses to rosuvastatin in Chinese patients. Pharmacogenet Genomics. Epub 2010 Jul 31 22. Bailey KM, Romaine SPR, Jackson BM, et al. Hepatic metabolism and transporter gene variants enhance response to rosuvastatin in patients with acute myocardial infarction: the GEOSTAT-1 study. Circ Cardiovasc Genet 2010; 3 (276-285) 23. Hall AS, Jackson BM, Farrin AJ, et al. A randomized, controlled trial of simvastatin versus rosuvastatin in patients with acute myocardial infarction: the secondary prevention of acute coronary events reduction of cholesterol to key European targets trial. Cardiovasc Prev Rehabil 2009 Dec; 16 (6): 712-21 24. Simonson SG, Martin PD, Mitchell PD, et al. Effect of rosuvastatin on warfarin pharmacodynamics and pharmacokinetics. J Clin Pharmacol 2005 Aug; 45 (8): 927-34 25. Martin PD, Warwick MJ, Dane AL, et al. A double-blind, randomized, incomplete crossover trial to assess the dose proportionality of rosuvastatin in healthy volunteers. Clin Ther 2003 Aug; 25 (8): 2215-24
2010 Adis Data Information BV. All rights reserved.
26. Martin PD, Warwick MJ, Dane AL, et al. Absolute oral bioavailability of rosuvastatin in healthy white adult male volunteers. Clin Ther 2003 Oct; 25 (10): 2553-63 27. Martin PD, Mitchell PD, Schneck DW. Pharmacodynamic effects and pharmacokinetics of a new HMG-CoA reductase inhibitor, rosuvastatin, after morning or evening administration in healthy volunteers. Br J Clin Pharmacol 2002 Nov; 54 (5): 472-7 28. Martin PD, Warwick MJ, Dane AL, et al. Metabolism, excretion, and pharmacokinetics of rosuvastatin in healthy adult male volunteers. Clin Ther 2003 Nov; 25 (11): 2822-35 29. Schuster H. Rosuvastatin a highly effective new 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor: review of clinical trial data at 10-40 mg doses in dyslipidemic patients. Cardiology 2003; 99 (3): 126-39 30. McCormick AD, McKillop D, Butters CJ, et al. ZD452: an HMG-CoA reductase inhibitor free of metabolically mediated drug interactions: metabolic studies in human in vitro systems [abstract no. 46]. J Clin Pharmacol 2000 Sep; 40 (9): 1055 31. Martin PD, Dane AL, Nwose OM, et al. No effect of age or gender on the pharmacokinetics of rosuvastatin: a new HMG-CoA reductase inhibitor. J Clin Pharmacol 2002 Oct; 42 (10): 1116-21 32. Lee E, Ryan S, Birmingham B, et al. Rosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residing in the same environment. Clin Pharmacol Ther 2005 Oct; 78 (4): 330-41 33. Zhang W, Yu B-N, He Y-J, et al. Role of BCRP 421C>A polymorphism on rosuvastatin pharmacokinetics in healthy Chinese males. Clin Chim Acta 2006 Nov; 373 (1-2): 99-103 34. Keskitalo JE, Zolk O, Fromm MF, et al. ABCG2 polymorphism markedly affects the pharmacokinetics of atorvastatin and rosuvastatin. Clin Pharmacol Ther 2009 Aug; 86 (2): 197-203 35. Cooper KJ, Martin PD, Dane AL, et al. The effect of erythromycin on the pharmacokinetics of rosuvastatin. Eur J Clin Pharmacol 2003 May; 59 (1): 51-6 36. Cooper KJ, Martin PD, Dane AL, et al. Lack of effect of ketoconazole on the pharmacokinetics of rosuvastatin in healthy subjects. Br J Clin Pharmacol 2003 Jan; 55 (1): 94-9 37. Cooper KJ, Martin PD, Dane AL, et al. Effect of itraconazole on the pharmacokinetics of rosuvastatin. Clin Pharmacol Ther 2003 Apr; 73 (4): 322-9 38. Cooper KJ, Martin PD, Dane AL, et al. The effect of fluconazole on the pharmacokinetics of rosuvastatin. Eur J Clin Pharmacol 2002 Nov; 58 (8): 527-31 39. Martin PD, Dane AL, Schneck DW, et al. An open-label, randomized, threeway crossover trial of the effects of coadministration of rosuvastatin and fenofibrate on the pharmacokinetic properties of rosuvastatin and fenofibric acid in healthy male volunteers. Clin Ther 2003 Feb; 25 (2): 459-71 40. Kosoglou T, Statkevich P, Yang B, et al. Pharmacodynamic interaction between ezetimibe and rosuvastatin. Curr Med Res Opin 2004; 20 (8): 1185-95 41. Gosai P, Liu J, Doyle RT, et al. Effect of omega-3-acid ethyl esters on the steady-state plasma pharmacokinetics of rosuvastatin in healthy adults. Expert Opin Pharmacother 2008 Dec; 9 (17): 2947-53 42. Schneck DW, Birmingham BK, Zalikowski JA, et al. The effect of gemfibrozil on the pharmacokinetics of rosuvastatin. Clin Pharmacol Ther 2004 May; 75 (5): 455-63 43. Kiser JJ, Gerber JG, Predhomme JA, et al. Drug/drug interaction between lopinavir/ritonavir and rosuvastatin in healthy volunteers. J Acquir Immune Defic Syndr 2008 Apr 15; 47 (5): 570-8 44. Busti AJ, Bain AM, Hall RG, et al. Effects of atazanavir/ritonavir or fosamprenavir/ritonavir on the pharmacokinetics of rosuvastatin (in 605-610]. J Cardiovasc Pharmacol 2008 Jun; (51): 6 45. Pham PA, la Porte CJL, Lee LS, et al. Differential effects of tipranavir plus ritonavir on atorvastatin or rosuvastatin pharmacokinetics in healthy volunteers. Antimicrob Agents Chemother 2009 Oct; 53 (10): 4385-92 46. Simonson SG, Raza A, Martin PD, et al. Rosuvastatin pharmacokinetics in heart transplant recipients administered an antirejection regimen including cyclosporine. Clin Pharmacol Ther 2004 Aug; 76 (2): 167-77
Am J Cardiovasc Drugs 2010; 10 (6)
400
Carter
47. Martin PD, Schneck DW, Dane AL, et al. The effect of a combination antacid preparation containing aluminium hydroxide and magnesium hydroxide on rosuvastatin pharmacokinetics. Curr Med Res Opin 2008; 24 (4): 1231-5 48. Martin PD, Kemp J, Dane AL, et al. No effect of rosuvastatin on the pharmacokinetics of digoxin in healthy volunteers. J Clin Pharmacol 2002 Dec; 42 (12): 1352-7 49. Simonson SG, Martin PD, Warwick MJ, et al. The effect of rosuvastatin on oestrogen & progestin pharmacokinetics in healthy women taking an oral contraceptive. Br J Clin Pharmacol 2003 Mar; 57 (3): 279-86 50. Ridker PM, Fonseca FAH, Genest J, et al. Baseline characteristics of participants in the JUPITER trial, a randomized placebo-controlled primary prevention trial of statin therapy among individuals with low low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein. Am J Cardiol 2007 Dec 1; 100 (11): 1659-64 51. Ridker PM, MacFadyen JG, Fonseca FAH, et al. Number needed to treat with rosuvastatin to prevent first cardiovascular events and death among men and women with low low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein: Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER). Circ Cardiovasc Qual Outcomes 2009 Nov; 2 (6): 616-23 52. Glynn RJ, Danielson E, Fonseca FAH, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med 2009 Apr 30; 360 (18): 1851-61 53. Everett BM, Glynn RJ, MacFadyen JG, et al. Rosuvastatin in the prevention of stroke among men and women with elevated levels of C-reactive protein: Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER). Circulation 2010 Jan 5; 121 (1): 143-50 54. Glynn RJ, Koenig W, Nordestgaard BG, et al. Rosuvastatin for primary prevention in older persons with elevated C-reactive protein and low to average low-density lipoprotein cholesterol levels: exploratory analysis of a randomized trial. Ann Intern Med 2010 Apr 20; 152 (8): 488-96 55. Mora S, Glynn RJ, Hsia J, et al. Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trials. Circulation 2010 Mar 9; 121 (9): 1069-77 56. Pradhan A, Glynn RJ, Ridker PM. Prevention of major cardiovascular events with rosuvastatin among patients with impaired fasting glucose: the JUPITER trial [abstract no. 1425]. Circulation 2009 Nov 3; 120 (18 Suppl. 1): S500 57. Ridker PM, MacFadyen J, Cressman M, et al. Efficacy of rosuvastatin among men and women with moderate chronic kidney disease and elevated highsensitivity C-reactive protein. J Am Coll Cardiol 2010 Mar 23; 55 (12): 1266-73 58. Ridker PM, MacFadyen J, Libby P, et al. Relation of baseline high-sensitivity C-reactive protein level to cardiovascular outcomes with rosuvastatin in the Justification for Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER). Am J Cardiol 2010 Jul 15; 106 (2): 204-9 59. Ridker PM, Genest J, Boekholdt SM, et al. HDL cholesterol and residual risk of first cardiovascular events after treatment with potent statin therapy: an analysis from the JUPITER trial. Lancet 2010 Jul; 376 (9738): 333-9 60. Ridker PM, Danielson E, Fonseca FAH, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 2009 Apr 4; 373 (9670): 1175-82 61. Ridker PM, Rifai N, Clearfield M, et al. Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events. N Engl J Med 2001 Jun 28; 344 (26): 1959-65 62. Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels. JAMA 1998 May 27; 279 (20): 1615-22
63. Shepherd J, Vidt DG, Miller E, et al. Safety of rosuvastatin: update on 16,876 rosuvastatin-treated patients in a multinational clinical trial program. Cardiology 2007; 107 (4): 433-43 64. The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med 2006 Aug 10; 355 (6): 549-59 65. Kahn R, Robertson RM, Smith R, et al. The impact of prevention on reducing the burden of cardiovascular disease. Circulation 2008 Jul 29; 118 (5): 576-85 66. National Cholesterol Education Program. Your guide to lowering your cholesterol with TLC [online]. Available from URL: http://www.nhlbi.nih.gov/ health/public/heart/chol/chol_tlc.pdf [Accessed 2010 Sep 7] 67. Buckley DI, Fu R, Freeman M. C-Reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann Intern Med 2009 Oct 6; 151 (7): 483-95 68. Michos ED, Blumenthal RS. Prevalence of low low-density lipoprotein cholesterol with elevated high sensitivity C-reactive protein in the U.S.: implications of the JUPITER (Justification for the Use of statins in primary Prevention: in Intervention Trial Evaluating Rosuvastatin) study. J Am Coll Cardiol 2009 Mar 17; 53 (11): 931-5 69. Plaisance EP, Grandjean PW. Physical activity and high-sensitivity C-reactive protein. Sports Med 2006; 36 (5): 443-58 70. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation 2002 Mar 5; 105 (9): 1135-43 71. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice. A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003 Jan 28; 107 (3): 499-511 72. Libby P, Crea F. Clinical implications of inflammation for cardiovascular primary prevention. Eur Heart J 2010 Apr; 31 (7): 777-83 73. Glynn RJ, MacFadyen JG, Ridker PM. Tracking of high-sensitivity C-reactive protein after an initially elevated concentration: the JUPITER Study. Clin Chem 2009 Feb; 55 (2): 305-12 74. Koenig W. Is hsCRP back on board? Implications from the JUPITER trial. Clin Chem 2009 Feb; 55 (2): 216-8 75. Ridker PM, Buring JE, Cook NR, et al. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14 719 initially healthy American women. Circulation 2003 Jan 28; 107 (3): 391-7 76. Ridker PM. Testing the inflammatory hypothesis of atherothrombosis: scientific rationale for the cardiovascular inflammation reduction trial (CIRT). J Thromb Haemost 2009; 7 Suppl. 1: 332-9 77. Danchin N. Rosuvastatin, C-reactive protein, LDL cholesterol, and the JUPITER trial [letter]. Lancet 2009 Jul 4; 374 (9683): 24-5 78. Jackson G, Citrome L. JUPITER: wake up and smell the coffee the absolute and relative merits of statin use. Int J Clin Pract 2009 Mar; 63 (3): 347-8 79. Mitka M. Studies examine inflammatory biomarker in prevention and prediction of heart disease. JAMA 2009 Jan 7; 301 (1): 23-4 80. Peters SAE, Palmer MK, Grobbee DE, et al. C-reactive protein lowering with rosuvastatin in the METEOR study. J Intern Med. Epub 2010 Mar 6 81. Crouse JR, Raichlen JS, Riley WA, et al. Effect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: the METEOR trial. JAMA 2007 Mar 28; 297 (12): 1344-53 82. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010 Feb 27; 375 (9716): 735-42
Correspondence: Natalie J. Carter, Adis, a Wolters Kluwer Business, 41 Centorian Drive, Private Bag 65901, Mairangi Bay, North Shore 0754, Auckland, New Zealand. E-mail: demail@adis.co.nz
Am J Cardiovasc Drugs 2010; 10 (6)
2010 Adis Data Information BV. All rights reserved.
You might also like
- Role of Oral Anti Diabetic DrugsDocument27 pagesRole of Oral Anti Diabetic DrugsjaidelindNo ratings yet
- Animal and Translational Models for CNS Drug Discovery: Reward Deficit DisordersFrom EverandAnimal and Translational Models for CNS Drug Discovery: Reward Deficit DisordersRobert A. McArthurNo ratings yet
- Duloxetine: Clinical Pharmacokinetics and Drug InteractionsDocument14 pagesDuloxetine: Clinical Pharmacokinetics and Drug InteractionsMario HBNo ratings yet
- Dyslipoproteinemia - Strategies for Diagnosis and TherapyFrom EverandDyslipoproteinemia - Strategies for Diagnosis and TherapyNo ratings yet
- Clinical Pharmacokinetics Volume 50 Issue 2 2011 (Doi 10.2165/11534750-000000000-00000) DR Garry G. Graham, Jeroen Punt, Manit Arora, Richard O. Day, Ma - Clinical Pharmacokinetics of MetforminDocument18 pagesClinical Pharmacokinetics Volume 50 Issue 2 2011 (Doi 10.2165/11534750-000000000-00000) DR Garry G. Graham, Jeroen Punt, Manit Arora, Richard O. Day, Ma - Clinical Pharmacokinetics of MetforminRob Sandoval StebanNo ratings yet
- Retention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsFrom EverandRetention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsNo ratings yet
- Nutritional ManagementDocument315 pagesNutritional ManagementOctavianus KevinNo ratings yet
- Barbara BeckDocument300 pagesBarbara BeckloristurdevantNo ratings yet
- Guia de MielomaDocument57 pagesGuia de MielomaVerónica Gabriela Pacheco PilcoNo ratings yet
- Similar But Not The Same Differential Diagnosis of HLH and SepsisDocument12 pagesSimilar But Not The Same Differential Diagnosis of HLH and SepsisJuan JoséNo ratings yet
- Coordination Chemistry Reviews: Luigi Messori, Antonello MerlinoDocument23 pagesCoordination Chemistry Reviews: Luigi Messori, Antonello MerlinoFelipe BrondaniNo ratings yet
- EPA-HQ-OPP-2009-0361-0073 - ContentDocument216 pagesEPA-HQ-OPP-2009-0361-0073 - ContentcroccocarmineNo ratings yet
- The International Journal of Biochemistry & Cell BiologyDocument15 pagesThe International Journal of Biochemistry & Cell BiologyNathalia PietraniNo ratings yet
- Farmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Document46 pagesFarmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Maria Marina Papaginovic LeivaNo ratings yet
- Medical treatment and operative repair of abdominal aortic aneurysmsFrom EverandMedical treatment and operative repair of abdominal aortic aneurysmsNo ratings yet
- PTSD Neuroimaging Fmrishin ModelDocument13 pagesPTSD Neuroimaging Fmrishin ModelSyifa MunawarahNo ratings yet
- Animal and Translational Models for CNS Drug Discovery: Neurological DisordersFrom EverandAnimal and Translational Models for CNS Drug Discovery: Neurological DisordersRobert A. McArthurNo ratings yet
- Garnock-JonesDocument28 pagesGarnock-JonesMary FallNo ratings yet
- 2020 Paterson Mich M SCRDocument182 pages2020 Paterson Mich M SCRZahra Al LawatiNo ratings yet
- Prevention and Treatment of Atherosclerosis 04 LDL Cholesterol Lowering TheraphyDocument29 pagesPrevention and Treatment of Atherosclerosis 04 LDL Cholesterol Lowering TheraphyHenry wijaya oeijNo ratings yet
- Pharmacist Quick Tips 2019-2Document31 pagesPharmacist Quick Tips 2019-2Setareh SepahiNo ratings yet
- AHA ACC Test Ergo Met RicoDocument56 pagesAHA ACC Test Ergo Met RicoValentina VaccaroNo ratings yet
- Sorkin 1987Document50 pagesSorkin 1987Galuh EkaNo ratings yet
- Pnds CBP VF HasDocument61 pagesPnds CBP VF HasDarck FairyNo ratings yet
- Smart Nanocarriers Bearing Docetaxel for Improved Chemotherapy CancerFrom EverandSmart Nanocarriers Bearing Docetaxel for Improved Chemotherapy CancerNo ratings yet
- VickeryR PDFDocument145 pagesVickeryR PDFOtrovanjeNo ratings yet
- Bupropion 3Document37 pagesBupropion 3Robert MovileanuNo ratings yet
- Endocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersFrom EverandEndocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersNo ratings yet
- Deficiencies of the Urea Cycle - Clinical Significance and TherapyFrom EverandDeficiencies of the Urea Cycle - Clinical Significance and TherapyNo ratings yet
- Murillo de Oliveira Antunes 2020Document15 pagesMurillo de Oliveira Antunes 2020Asisten Lab TLPNo ratings yet
- FaR-RMS Protocol Version 2.0b - 06thdec2021Document187 pagesFaR-RMS Protocol Version 2.0b - 06thdec2021Alina CretuNo ratings yet
- Handbook of Essential Pharmacokinetics, Pharmacodynamics, and Drug Metabolism For Industrial ScientistDocument302 pagesHandbook of Essential Pharmacokinetics, Pharmacodynamics, and Drug Metabolism For Industrial Scientistdavid_dung100% (2)
- Piracetam and Piracetam Like Drugs From Basic.4Document26 pagesPiracetam and Piracetam Like Drugs From Basic.4jsoriano6No ratings yet
- MDMA-IB-15th-Edition FINAL 13MAR2023 MRCDocument200 pagesMDMA-IB-15th-Edition FINAL 13MAR2023 MRCSi MarNo ratings yet
- A Review On Plant-Based Rutin Extraction Methods and Its Pharmacological ActivitiesDocument13 pagesA Review On Plant-Based Rutin Extraction Methods and Its Pharmacological ActivitieswahyuniNo ratings yet
- Professional Development: A Guide for Primary CareFrom EverandProfessional Development: A Guide for Primary CareMargareth AttwoodNo ratings yet
- The Antioxidant and Anticancer Potentials of New Zealand Manuka Honey and Thyme HoneyDocument128 pagesThe Antioxidant and Anticancer Potentials of New Zealand Manuka Honey and Thyme Honeyمنير علي هباطيNo ratings yet
- CMA Drivers Guide 8th Edition eDocument148 pagesCMA Drivers Guide 8th Edition eNeil NaikNo ratings yet
- JG02 v1-0 10apr10 W507 Student Manual1 PDFDocument213 pagesJG02 v1-0 10apr10 W507 Student Manual1 PDFHerna S Hasugian100% (1)
- Smoking Guidelines - enDocument191 pagesSmoking Guidelines - endhwanit31No ratings yet
- Manual PDFDocument149 pagesManual PDFCoria AndresNo ratings yet
- Polyphenols For Cancer TherapyDocument19 pagesPolyphenols For Cancer TherapySpore FluxNo ratings yet
- AABB Circular of Information For CTDocument30 pagesAABB Circular of Information For CTSenthil ThyagarajanNo ratings yet
- Ketamine JaffdispubDocument12 pagesKetamine JaffdispubT Smith AndresNo ratings yet
- N207917 Adapalene and Benzoyl Peroxide Clinical PREA 2 PDFDocument49 pagesN207917 Adapalene and Benzoyl Peroxide Clinical PREA 2 PDFKing MatNo ratings yet
- Protein Aggregation and Inhibition in Bio PharmaceuticsDocument30 pagesProtein Aggregation and Inhibition in Bio PharmaceuticsFatima Herranz Trillo100% (2)
- Cma Drivers Guide 8th Edition eDocument148 pagesCma Drivers Guide 8th Edition eapi-285271906No ratings yet
- Methamphetamine PsychosisDocument138 pagesMethamphetamine Psychosisamalda06100% (1)
- Newborn Screening Manual of Operations v2019Document86 pagesNewborn Screening Manual of Operations v2019Enrico SocoNo ratings yet
- Sakai Et Al-2019-Cochrane Database of Systematic ReviewsDocument47 pagesSakai Et Al-2019-Cochrane Database of Systematic ReviewsNakarit SangsirinawinNo ratings yet
- Acute Myeloid LeukemiaDocument45 pagesAcute Myeloid Leukemiasabila nugraha100% (1)
- Searching For Hypothetical ProteinsDocument38 pagesSearching For Hypothetical Proteinssumera120488No ratings yet
- Tracking Medicine - John E. WennbergDocument340 pagesTracking Medicine - John E. WennbergurbanincultureNo ratings yet
- Manual CTO Ginecologia 7 EdicionDocument102 pagesManual CTO Ginecologia 7 Edicioncharly476100% (2)
- Survival - First Aid For SoldiersDocument304 pagesSurvival - First Aid For SoldiersurbanincultureNo ratings yet
- Telmisartan Amlodipine Single Pill Combination In.6Document12 pagesTelmisartan Amlodipine Single Pill Combination In.6urbanincultureNo ratings yet
- Wolff-Parkinson-White ECGDocument1 pageWolff-Parkinson-White ECGurbanincultureNo ratings yet
- Twiddlers Syndrome An Unusual CauseDocument2 pagesTwiddlers Syndrome An Unusual CauseurbanincultureNo ratings yet
- Genuine (Ly) Unreliable Passports: How To Obtain A Second IdentityDocument2 pagesGenuine (Ly) Unreliable Passports: How To Obtain A Second IdentityurbanincultureNo ratings yet
- Spanish ACLS Provider Manual ErrataDocument2 pagesSpanish ACLS Provider Manual ErrataurbanincultureNo ratings yet
- Supplement 2 TS Warehouse Design ECSPP ECBSDocument36 pagesSupplement 2 TS Warehouse Design ECSPP ECBSBendis Bendis100% (1)
- ClandestineDocument85 pagesClandestineeryan_costa15680% (1)
- Jerin SangroseDocument37 pagesJerin SangroseVishnu NairNo ratings yet
- Consumer Insight and SegmentationDocument2 pagesConsumer Insight and SegmentationDatheshNo ratings yet
- Modern Pharmaceutics 4th Edition Chapter 10Document47 pagesModern Pharmaceutics 4th Edition Chapter 10Faysal MasoodNo ratings yet
- Antifoams ChartDocument1 pageAntifoams ChartTariq Khan OtmanzaiNo ratings yet
- Nclex - Drug Dosage Calculations Practice Exam 1Document8 pagesNclex - Drug Dosage Calculations Practice Exam 1Angie Mandeoya100% (2)
- Management of PatientsDocument19 pagesManagement of PatientsAmin MasromNo ratings yet
- Herbal MedicineDocument6 pagesHerbal MedicineMprado DelgadoNo ratings yet
- Chapter 1Document23 pagesChapter 1Kuia AllardeNo ratings yet
- Solvent List For PolycaprolactoneDocument8 pagesSolvent List For Polycaprolactonedibyodibakar100% (2)
- A New Generation of Liposome PDFDocument26 pagesA New Generation of Liposome PDFJ C Torres FormalabNo ratings yet
- A Paradigm Shift in The Management of AsthmaDocument3 pagesA Paradigm Shift in The Management of AsthmaRuqayya AdamuNo ratings yet
- Article 017Document10 pagesArticle 017Digambar GondvaleNo ratings yet
- MSQH Survey Recomendation PDFDocument2 pagesMSQH Survey Recomendation PDFChristine TanNo ratings yet
- Anti Leprosy Drug SeminarDocument76 pagesAnti Leprosy Drug SeminarSiddharth DashNo ratings yet
- Save Time With Magellan RX Home: Obtain Your Maintenance Medications by MailDocument3 pagesSave Time With Magellan RX Home: Obtain Your Maintenance Medications by MailwalterbircherNo ratings yet
- Affliated To Gautam Buddh Technicaluniversity Lucknow,: AcknowledgementDocument41 pagesAffliated To Gautam Buddh Technicaluniversity Lucknow,: AcknowledgementGaurav JaiswalNo ratings yet
- Assay of Alkaloid and Amine DrugsDocument3 pagesAssay of Alkaloid and Amine DrugsKate Lorraine Arnigo MercadoNo ratings yet
- Medication GuidesDocument38 pagesMedication GuidesEko YuliantoNo ratings yet
- What Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantDocument3 pagesWhat Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantthegroovyNo ratings yet
- 2011-12 B.tech. Cosmetic IIIDocument19 pages2011-12 B.tech. Cosmetic IIINilesh B ChaudhariNo ratings yet
- Challenges and Opportunities in The Encapsulation of Liquid and Semi Solid Formulations Into Capsules For Oral AdministrationDocument16 pagesChallenges and Opportunities in The Encapsulation of Liquid and Semi Solid Formulations Into Capsules For Oral AdministrationLathifatus ShalihahNo ratings yet
- AmphetaminesDocument11 pagesAmphetaminesMatt CrossNo ratings yet
- Benzodiazepines in General PDFDocument18 pagesBenzodiazepines in General PDFmartacarlosNo ratings yet
- Adrenergic Drugs (Sympathomimetics, Adrenomimetics)Document43 pagesAdrenergic Drugs (Sympathomimetics, Adrenomimetics)cancivNo ratings yet
- Pharmaceutical Calculation - Pacop BlueDocument31 pagesPharmaceutical Calculation - Pacop BlueSophia AndresNo ratings yet
- PMP Alkaloids PDFDocument5 pagesPMP Alkaloids PDFjigoooNo ratings yet
- Sepha White Paper Non Destructive VisionScanDocument12 pagesSepha White Paper Non Destructive VisionScananshulNo ratings yet
- Resume Book: Columbia Healthcare and Pharmaceutical Management ProgramDocument44 pagesResume Book: Columbia Healthcare and Pharmaceutical Management ProgramJohn Mathias100% (2)