METRO MANILA
DEVELOPMENTAL SCREENING
TEST MANUAL
[PHOEBE DAUZ WILLIAMS, RN, PhD *
ADELINA B. ABAD SANTOS, RN, MN
LUZ B. TUNGPALAN, RN, MA
JOSEFINA A. TUAZON, RN, MN
Editors
Research and Creative Writing Program
ORNURSING
=e ‘of the Philippines paanila
Kins b FO days
befual: ge
Lab 5 Ted:
Sihdab: 2/e 12
8
# (2 «te panstaty)
Metro Manila Developmental serning Test Manual
‘Second Eilon
Copyright © 1999
by University ofthe Philipines Manila College of Nursing
First Eition, 1985
aitors: Adelina B. Abed Santos
Luz B. Tungpalan
All rights reserved. No part ofthis work covered by copyright
herein may he reproduced or copied in auy form or by any means
‘without written permission of the publisher
Published by’
University ofthe Philipines Manila
College of Nursing
Pedro Gil Sc, Malate, Manila
Philippines
523-1472/523-1494,
a -
18B0/971-93085-07
wy 9 yole # yO.
Foreword /v
Preface /vi
Overview of the MMDST J 1
Test Form / 4
Preliminary Phase
Test Administration
‘Test Items: Administration and Scoring Directions J 15
Scoring Delays in Development / 66
Interpreting Test Results / 67
Discussing Test Results / 68
Retesting / 68
Difficult Test Situations / 69
Practice Testing / 73
References /74
Appendices /16
‘A. Sample Protocols /77
B. MMDST Administration Checklist / 81
C. Denver Developmental Screening Test / 83
Foreword
‘The Metro Manila Developmental Screening Test
(MMDST) devised by Dr. Phoebe Williams as a pediatric
Ssorecning test is a milestone in mursing. Being culture
based, it has been widely used by nurses, physicians and
other workers for nearly two decades now. Indeed, its
culture sensitivity makes it easy to use for Filipino
children.
_. The MOMS T is research-based and, as such, should be
inherent 10 nursing practice. Developmental screening
should be made an integral part of the nursing curriculum
to enhance the competency of professional nurses,
specially would-be child health nurses, family nurse
practioner and nurse specialists.
‘The publication of this revised edition is part of the
UP. College of Nursing's commitment towards
professional advancement in nursing and the enhancement
‘of the Filipino nurse’s involvement in promoting wellness,
and preventing disability.
‘This project has been made possible with the support of
the Commission on Higher Education (CHED) in
recognition ofthe UPCN’s role as a center of excellence in
nursing education,
= lnpiten Wi dared
CORN LAURENT Tat
Dean UP. Calloge of uring
Preface
‘This manual describes a screening process using the Metro
‘Manila Developmental Sereening Test (MMDST). ‘This test
was the product of a normative study in 1980 by the author,
Dr. Phoebe Dauz Williams, on Metro Manila children to
standardize the widely recognized Denver Developmental
Screening Test of Prankenburg and his associates: Since then,
the MMDST has been validated and well ulilized not only in
research but in practice as well by aurses, pediatricians and
other health workers. Today, William's MMDST remains to
bbe the recognized developmental screening test among
Filipino children
“The author is a nurse researcher and professor with a BS in
‘Nursing and MA in Psychology from the University of the
Philippines, and Masters in Nursing and PhD from the
University of Pittsburgh. She was a former professor and
hhead of the Department of Research, University of the
Philippines College of Nursing. She is currently Professor of
the University of Kansas School of Nursing and the only
Filipino Fellow of the Americen Academy of Nursing
(FAN). Although she has been abrond for almost two
decades now, she remains to be an active member of the U.P.
College of Nursing. From across the miles, she produced the
first edition of the MMDST Manual in collaboration with the
“UPCN Department of Research in 1985. Adelina B: Abad
Santos and Luz B. Tungpalan edited this first edition,
~~
‘This second edition of the MMDST Manual isa project
of the Research and Creative Writing Program of the UP
College of Nursing, just as the fist edition was. This edition
promises a format and language that is userriendly. Its
‘more compact size makes it handier that will fit snugly into
the MMDST bag with the test materials, The topics have
also been rearranged for easier comprehension. Some of the
illustrative examples were updated and made consistent with
the test form for better integration of learning,
‘This project isthe result ofa collaborative effort of many
people. We specially acknowledge the editorial expertise of
Prof, Luz B. Tungpalan whose assistance was invaluable,
and to the editorial staff, Sheila R. Bonito who prepared the
manual for publication with the assistance of Erlinda S.
Bilog and Glorie €. Mangalino. Special mention has 10 be
sven to Prof. Ma, Estela M. Layug whose expertise in the
_MMMNCT nod tuable comments helped direct the revisions
‘undertaken. Lastly, this project would never have reached
this stage without the urging and support of Dean Cecilia M.
Laurent.
‘The project of writing the second edition is a personal
fulfillment because as a young graduste, my first job was as
‘research assistant to Dr. William’s normative study. And
itis a privilege for RCWP to be given the chance to be a
collaborative partner with the likes of Dr. Williams and
Prof. Tungpalan,
Josefina A. Angeles Tuazon
Head, Research and Creative
Writing Program (RCWP)
December 1999
An Oversiew
Screening is the presumptive identi
‘unrecognized disease or defect by the applicatic
‘examinations or other procedures that can be applied rapidly.
Screening tests sort out apparently well persons who
probably have the problem from those who probably do not,
permitting those with positive or suspicious findings to be
referred for diagnosis and appropriate treatment as early as
possible. One such screening tést is the Metro Manila
Development Screening Test (MMDST). It is an. carly
detection model that applies to the detection of developmental
ties in children aged six and a half years old and
=T“8-98T is simple-cinically useful tool used in the
carly detection of children with serious developmental delays
developed by Dr. Phoebe D. Williams. It is a modification and
standardization of the original Denver Developmental
Screening Test (DDST) by Dr. William K. Frankenburg
and his associates (1970) on 6,006 Metro Manila children. It
‘was developed for health professionals such as nurses, doctors
and other health workers so that slow development may be
recognized, referals made, and approprite therapy prescribed
1s soon as possible. Just like the DDST, the MMDST is not an
intelligence test. It is intended as a screening instrument to
determine whether 2 child’s development is within normal
range,
‘The MMDST is designed to detect developmental delays in
children 2 weeks fo 6 4 years old. It evaluates four aspects of
4 child’s development: personal-social, fine motor-adaptive,
tos Moret
“The test is administered using the MMDST kit which
includes the manual, sample test form, test materials and the
MMDST bag. The test materials are standard and shown in
Figure 1. These consist of the following:
+A bright red yarn pom-pom
© Aratte with a narrow handle
Eight 1-inch colored wooden blocks
(fed, blue, yellow, green)
+A small clear glass/bottle with 5/8 neh opening,
+A small bell with 2 % ineh-diameter mouth
+ Arubber ball 12 inches in circumference
= Cheese curls
+ Apencil
+ Bond paper
CCaleutating the child's age-and-indicating the age line is
crucial, if not the most important, initial step in test
‘administration. The test items that will be administered will
‘depend on the calculated age of the child, Therefore, this will,
guide the selection of test items to be administered and the
subsequent interpretation of the MMDSTT results.
Four kinds of scores may be given for eact test item:
‘passed, failed, refused ot no opportunity. Failure of an item
that is completely to the left of the child's age line is
‘considered a developmental delay and is therefore referred to
inthe MMDST as a delay
‘The succeeding sections of this manual will describe the
test form, steps in administering the MMDST, scoring each
test item, and interpreting the test. Difficult test situations are
also presented plus the conditions under which retesting is
Saceeptable.
Figure 1, Test Materials
rte
ost Mae
Like the DDST, the MMDST is made up of 105 items
wwttten in the range of accomplishments for children between
birth and six years of age, The sample test form is shown in
Figure 2. Instructions for administering footnoted items are
placed at the back of the test form. These items are
‘categorized in four sectors:
I, Personal-Social - tasks which indicate the child's
ability to get along with people and to take care of
himself.
2. Fine Motor-Adaptive - tasks which indicate the child's
ability to see and to use his hands to pick up objects and
to draw. °
3. Language - tasks which indicate the child's ability to
hear, follow directions and to speak; and
4. Gross Motor - tasks which indicate the child's ability
to sit, walk, and jump,
Across the top and bottom ofthe test form are age scales
raking ape in moaths frm I 024, and ages in yeas froma
| Bite G. Each of the test items i epresented inthe et form
bya ba The bar is placed along the age scale to show when
Bes, s0% (indicated by the hatch mack) 75% and 90% of
oma children ae able to pas the ilem. A sample est item
tnd ihe corresponding age sal is shown in Figure 3.
AGE SCALE (noitts)
i a, 6 18 20
7 atch mask
rece et 2506 19%
Saat, 2p So
Figure 3
Test Directions for Footnoted Items
1. ‘Try to get child to smile by smiling talking or waving to hin,
ao nol touch him
‘When child i playing with toy, pli aay ftom him. Pass if
he resists
Child does not have tobe able to tie shoes or button inthe bac,
4. Move yarn slovily in an arch fram one side tothe othe, about 6”
above chile’s fice. Pass if eyes follow 90° to midline. (Past
idling; 180°)
5, Pass if the child grasps rate when it is touched to the backs or
tips of fingers
6, Passif child continues to look where yam disappeared or tries to
see where it went. Yam shouldbe dropped quickly ftom sight
fiom tester's hand without arm movement.
7. Pass if child picks yp cheose curl with any part of thumb and
finger.
8. Pass if child picks up cheese curl with the ends of thumb and
‘nox finger using an over hand approach,
O |
9, Pass any en- 10, Which lite is 11. Passanyeross- 12. Have child
loged form. longer (aot ing ine copy
Pal comin. bigger. Turn Ir failed,
ous round paper upside demon
sotoes flown and 10 sete
peat GB or
5)
Whea giving items 9,11 and 12, do not name the forms, Do not
demonstrate 9 snd 11
13, When scoring, cach pair (2 arms.2 legs, ee:) counts as one par
14, Point to picture and have childname it. (No credit i piven. for
oer 5
/ Sree meee
we fae |
15, Tell child to: give block to Mommy; put block on tables put
block on floor, Pass 2 of 3. (Do nor help child by pointing.
‘moving head or eyes.)
16, Ask child: What do you do when you are cold? hungry? ied?
Pass 2 of 3.
17-Tell child to: Put block om able; under wble; in front of char,
behind chair. Pass 3 of & (Do nor help child by pointing,
moving head or eyes)
18, Ask child: If fire is hot, ice is?; Mother is a woman, Dad isa;
‘horse isi, a mouse is? Pass 2 of 3.
19, Ask child: What isa ball? iver? desk? house? banana? cuts?
roof? fence? street? Pass if defined in terms of use, shape, what
itis made of or its general category (such as banana is x rut, ot
just yellow). Pass 6 of 9.
20, "Ask ehild: What isa spoon made of? shoe made of
rade of? (No other objects may be eubsunued.) Pass 3 of.
21, When paced on stomach, child its chest off table with support,
of forearms and/or hands
22, While child is on his back, grasp his hands and pall him to
siting. Pass if ead does not hang back.
23, Child may use wal or rail only, net person. May nt craw
24 Child must throw ball overbead 3 fet to within arm's reach of
tester.
25. Child must perform standing bread jumps over width of test
sheet (8 % inches).
26, Tell eld to walk forward, DEDEDE —P heel within
inch of toe. Tester may demonstste, Child must walk
consecutive steps, 2 out of 3 tals
27, Bounce ball to child who should stand 3 feet away form tester.
(Child mast cate ball with hands, not amas, 2 out of 3 rials
26, Tell child to walk backward @-©DeqeDeqy toe within
inch of heel. Tester may demonstrate. Child must walk 4
consecutive steps, 2 out of 3 tials.
DATE AND EITAYIORAL OBSERVATIONS (ow il nef ens
Tots, aeton posal bow eee ee)
“The bar representing the item, waiks well, in Figure 3 is
located between ages less than 12 mouths and 17 months. The
Jeft end of the bar denotes that 25% of normal children walk
‘well at less than 12 months, 50% (indicated by hatch mark) at
13 V4 months, le end of shaded area shows 75% do so at 15,
‘months, and right end of bar shows 90% walk well at about 17
‘months. All est tems are represented similarly.
+ Some test items have a smal footnote number at the left end
‘of the bar. This number indiestes the corresponding instruction
for administering the item that is found at the back of the fest
form (see Figure 2). For example, the instruction for the item,
‘walks up steps, is #23 at the back of the test form (see Figure
4.
Some test items may be passed by report of the parent.
‘The leterR in the bar as shown in Figure 4 indicates this. Only
items with an R on the form may be passed by report. Howes,
‘whenever pase the teser shoul obsave vat the child can actually
perform rather than ask the parent, even though the item may
‘be passed by report.
ne in
oe
Figure 4
‘The iter, equal movements, as an asterisk (*) at the right
end of ts bar, This indicates that 100% of normal children pass
this item at birth. The item is hardly seen in the form but itis
the only item wit an * and is located in the fine motor adaptive
sector ofthe test form.
‘Nine items have arrows (->) atthe right end of these bars.
‘This includes the items, defines words and composition of _.
‘The-arra atnormia-children-may-pass these items
even beyond 6: reas of age.
Caleulating the Child’s Age
‘The fist step is to calculate the child’s age. ‘This will be the
basis for drawing the age line later and determining the test
items to be administered. Check the calculation very well
before placing the age line on the form
[Ask forthe birth date of the child and calculate the exact age
using this formula: date of test minus birth date equals age of
child, Caloulate first the days, then months, and then years. To
iMustrate, ifthe birth date is Mareh 10, 1997 and the date of test
is November 27, 1999; then:
. Year ‘Month Day
Date of Test 89 4 15
Birth date 7 3 -10
‘Age of Child z 5 3
‘Age of this child is therefore 2 years 8 months and 15 As an ieebreaker, offer the child a cheese curl or give
him @ block, a bell or a rattle to play with prior to
testing.
+ Start testing with ites that are scored by report. Fo-
ccusing attention initially on the parent gives the child a
chance to cope with the situation and becomes more
familiar with the tester and the test materials.
If the child remains shy and wary, ask the parent £0
‘administer some ofthe test items or show how they are
done. Asthe parent demonsrates, you can say, “Tigran
fro nga hurg makalalakad ka din ng paurong gaya ng
onay mo.” Preschoolers are grest show-offs. This
technique ray work and if does, reinforce the child
forperforwine
TF miggesthe-ui ad U8 TOTES not Complet, retest 2
or 3 weeks ler.
-o
os Maat
The Uncooperative Child
‘The uncooperative child is one who is not shy but
refuses to do what is asked of him/her. Approaches for the
shiy chile may also be applied t0 the uncooperative child. In
addition, the following may be trie:
‘+ Ask the parent to leave the room. The chile may perfonn
beter in the pirent’s absence. Anxious felings of a parent
are communieted tothe child who in tum acts negatively.
+ the child becomes upset by the separation, the parent
need not leave the oom but is requested to tum away
“while staying within seeing distance ofthe child
«Ifthe parent says thatthe child can do certain items but
js just uncooperative, ask the child to do the opposite.
Reverse psychology often works inthe negativistc age
You might say, “Sa palagay ko, hind ka marunong
magdrawing ng. tao.”
The Overactive Child
‘An overactive child is one whose interest shifts rapidly
from one test item/material to anothet. He/she may be
seated beside you building blocks and as you tura to consult
the test form, the child sees the ball in the kit, drops the
blocks, gets the ball and runs off with i. Getting him to sit
ddovin to continue the testis’ chore. While you may succeed
in getting him to perform again, the attention span is short.
Dealing with an overactive child may be a difficult
experience to the child, the parent and the tester. ‘There are
‘ways, however, of dealing with this situation
+ Mastery of test items ~ based on the example given
above, when the child drops the blocks and picks up the
ball, be ready 10 test him on other items: "Spain mo
tong bola." Qnoe done, follow with “Saluhin mo ito.”
ee ee ae himon
0st Nay
recognition of colors. ‘The sequence of testing may be
jumbled depending on the situation. If the tester has.
mastered the test form, jumping from one sector to an-
other is easy
Limit the distractions ~ clear the room of al distractions.
If this is not possible in crowded places (home, clini oF
health center), arrange the table and the child's position on
the table in such away that hisher back i tothe distrac-
tion
Bring out only the tpst materials needed per item. Keep
the rest in the bag and do not give the child chance to see
its contents or else he/she may not rest until he gets hold
of everything. *
‘Another technique to is keep the bag behind you, leave it
‘open, and reach forthe test materials as needed. As you
{do this, mainten oye contact with the child at all times to
hold his atentian. 2
‘An older child is usually wiser and may realize that that
you are hiding things as you fumble through the bag. If
iis happens, tel the child that you have a series of
surprises (young children love surprises) for hinvher but
{hat helshe has tobe very attentive and follow directions.
Direct the child’s etention gain the child’s attention
‘Once obtained, focus iton the task to be performed. If
attention lags, cll him by name or touch his arm gently 10
‘ring him back to the task at hand,
Be firm and calm ~ Filipino chiléren, including the ove
active, respond to authority. Uniformed people like
nurses, doctors and policemen are usually held in awe.
Firm bat calm words from these people often work wire
parents fail, TELL the child what to do, DO NOT ASK
ithe can or if he will perform the task
FE PORTIS, ols the-chwlé-on your laps
hiner. This way, 11 easier to comry!
‘The Chitd with many Siblings
{is sometimes difficult to contol the situation in homes
\with many siblings. Each child wants to perform the tasks
all at the same time; or, a child already done with the test
tells the other what to do. Ascendant behavior or bossiness|
begins at around age 3. A desire to excel is manifested as
carly:as age 4. In this situation, explain to the mother the
need to test each child individually. As each child, prefer-
ably starting with the eldest, accomplishes the test, ask the
nother to send the child on errands, This technique keeps:
hhim put of the way, thus giving the remaining children 2
chance to perform on their own, without comments or
prompting from others. z
The Interfering Pares
‘The interfering parent is ene who becomes too involved
“This parent answers the questions for the child and shows
him what to do,
‘The following techniques are suggested:
a, Explain to the parent, as inal west situations, that
the MMDST is not an intelligence test and that
the child is not expected to pass all the items.
‘The test will only show what the child can do at
‘certain age. Be sure the mother understands the
purpose ofthe test
‘Administer the test
If the parent interferes, repeat the explanation as
4. If the parent still tells the child what to do,
Frankenburg suggests that the parent leave the
room. A face-saving way is to discontinue the
test. Then reset the discontinued test for re
sereeging within 2 or 3 weeks. -Score the items
by nyport of interfering parents with eare. They
may
tbe reliable.
soos nt
“The administration of the MMDST requires practice to
develop an acceptable level of competency. The tester should
bbe competent 10 obiain valid test results. Its therefore recom
mended tat beginning users ofthis screening test ot only practice but
also have someone to evaluate their competency using the MMDST
‘Administration Cheeklist provided in Appencix B.
Williams’ slide-tape program is availsble that you can view
prior to practice and actual administration of the MMDST. If
Frankenburg et e.s proficiency training film is available or its
equivalent, view this also and compare your performance with
the expected answers, Proficiency on the DDST/Denver Il i a
requirement for pediatric and family nurse practitioners in the
United States. =
When you do your practice, perform the test on children
with Warioasages eerste; yacte skill: The following has
‘been recommended inthe original DDST:
4 chiléren between | month and 9 months of ages
4 children between 9 months and 2 years of age: and
4 children berweon 2 years and 6 years of age
It is helpful to pair off with another person to practice test.
[As one person tests, another observes and uses the checklist
‘The observer should discuss anything omitted by the tester and
any disagreements in administration or scoring to the manual
and/your instructor to settle any difference.
‘After practice testing with at least 12 children, ask your
instructor or test partner fora reliability testing session. This is
‘done with you administering the test om one to three children
(of the age ranges stated above) and your instructon/partner
independently scoring the test as you administer it. You should
cobtain-ot Jegst 90% agrooment, with your instruptorpartner, If
noi, Tid out Uievareas of disagreement and s, delice in those
‘areas, Repeat the reliability testing session, if deeded.
oss Ment
References
[Abad Santos, AB (1980). An Analsisof Figure Drawing of Mets
‘Manila Preschoo!Chiléen. to P. Wiliams (ed), Development
‘of Norm for the Denver Developmental Sercening Test on
‘Metro Manila Children 046 Years Old, pp115-198 NSDB-UPS
a
Anasasiow, N., Grimmett, 8 Eggleston, P., and Brown. (197).
aciltative Environments Encouraging Development (FEED)
=. lsttte for Child Study, Indiana University, Bloomington,
Frankenborg, W. & Fandall, A, Dodis, J, (1970). Deaver
Developmental Sereening Test Manual " (Revised) Denver
University of Colorado Press
Frankenburg, W., Goldstein, A, Chabot, A., Camp, B.W, and Fitch,
IM. (1970). Traiing the Indigenous Nonprofesiont; The
Screening Technician J. Pediatries, 77 564-570.
‘rankenburg, WK, Camp, B.W, VanNets, PAA & Demersseman, 1A
(97a) Relihilty & Sabilty of the Denver Developmeatal
Screening Tes. Chilé Development, 423475485.
Guthrie, G., Tayag A, eobs,P. (1965) "The Philippine Non-Verb
Intlignce Test (PNIT) Manual, Philippine Normal College,
Manila
Layug, F. (1980). Concurrent Validation of the DDST (Meteo-
‘Manita version) Unpublished master's thesis, University ofthe
Philippines, Quezon City
Williams, PD. & Madiazo, CV. (1983) Early Wentiieation ofthe
‘Child at Risk: A Philippine Perspetive, Paper presented atthe
Fourth International “Conference on Early Ldenfcation
‘September 18-23, [983, owas, Colorado
/
PD, (1982) The Moto Manila Developmental Serening
"Testa Normative Sty”, Ip Anassiow, Nl Prankeaborg WK,
and Fandall A.W, Hdenifying the Developmentally Delayed
‘Chik, Batre: University Park Press
Wiliams, PD, (19803). Development of Norms for the Denver
‘Developmental Serening Test on Metro Manila Children. 0-6
‘Years Old. NSDB-UPS (A) Projet No. 703 So,
Winiams, PD. (1980b).'A. Comparative Study of DDST Norms
Developed in Five Locales. In: PD. Willams (Ed), Nursing
Reseach i the Philippines: a Sourcebook. IMC Press, Quezon
ciy «
‘Wiliams, PD” (1986). The Rellibilty ofthe Denver Developmental
Serening Test: Mero Manila version. In P. Willams (E3.)
Development of Norms for the Denver Developmental
Screening Test on Metro Mauils Chikiren 0-6 Years Old
[NSDB- (A) Projet No. 708 Sa, Append
Willams, PD. (980d). Predietive Valdty of the Metro Manila
Developmental Screening Test. Paper resented a the Philippine
Physiologie! Assocation Convention August 26, Manila
Wiliams, P1979) Unnarew at Rusk: Perinatal Event and heir
“Elects on Development: A Cross-Sectional Study. Unpublished
Wiliams, PD. & Williams, AR (1983) “Factors Affecting
‘Development of Filipino at Risk", preseoted at seminar on
‘Children at Risk: Aw International Perspective, University of
Colorado Health Ssinoes Contr, Denver. Colorado, September
16,1983,
Appendix A
SAMPLE PROTOCOLS
Normal Test Result
Abnormel Tést Result
Questionable Test Result
Untestable Test Result
1 woos-wnostea
NLEYOV HOLOM aN
yoi0H ss0us
ae
wr] Cee
T,t.7-$7
tas tials) 6
(0-1-8
sae, t
“
ae
FINE MOTOR ADAPTAE
PERGONAL-SOOIAL
"FINE woTOR ADAPTIVE
GM sector, 2 delays
FMA sector, I delay and
in that same sector no
pass intersects age line.
wicosrwnosuas
aniLavay WOUOIN 3s
vo1oH ssoun)
v
Appendix B
MMDST ADMINISTRATION.CHECKLIST
Purpose: This checklist should be used regularly until the
tester becomes proficient in administerhg the
‘MMDST.
Instructions: To. check the, accuracy of your own testing
ability, go over the checklist immediately after
you have finished giving a test. To check the
fceuraey of another person's test sidministra-
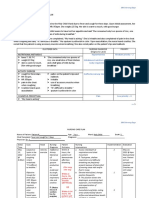
BEFORE THE TEST: CORRECT INCORRECT
1. Can child see and reach test
rome ean? Yo at
eee
2, Did the examiner expin at Ya Ne
fhe MIDST ine an IQs
3. Dit te ermine plas Bt ya, yp
childs ot expeced a por
form everything asked of him?
Epi ts Canker ekisoage ae ts
fehl er king pron
hiss bia?
5, Bee drag a2 ne, 4 yu
txaminer fh wes bom
emt?
6. Was age line drawn correctly? Y& ‘No
$ Divde emninerindiwe dete yyy
test was administered at top of
‘age line?
DURING THE TEST:
itd the examiner assure cooperation
of child by:
8, giving child a chance to become
used to examiner?
9. starting each sector of test with
items child could pass?
10.telling child what to do rather
than asking?
IL. Was table clear of materials
which were not being used?
12, When asking for parent's report,
did examiner suggest an answer
by the way question was
‘worded? (leading question)
13;Did the examiner praise child
only when he correctly per-
“formed an item?
14, At the ond of test, did the exam-
iner ask parent if behavior of
child was typical of his usual
‘behavior?
15, Did examiner administer enough
items? (At least 3 passes and 3
failures in each sector)
AFTER THE TEST,
16, Were delays emiphasized by
shading in right end of bar?
17. Were delays indicated only on
those items failed which were
completely to let of age line?
18, Was test performance interpreted
comectly?
19 Did the examiner write observa-
“S
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CHN 1 LEC - Family Nursing ProcessDocument7 pagesCHN 1 LEC - Family Nursing ProcessBea Abigail BrocalNo ratings yet
- 05b. Part 2 of Nucleic Acids For BSRadTechDocument26 pages05b. Part 2 of Nucleic Acids For BSRadTechBea Abigail BrocalNo ratings yet
- MMDSTDocument52 pagesMMDSTBea Abigail BrocalNo ratings yet
- STD SDocument2 pagesSTD SBea Abigail BrocalNo ratings yet
- STS 100 FinalDocument11 pagesSTS 100 FinalBea Abigail BrocalNo ratings yet
- Health Assessment MergedDocument154 pagesHealth Assessment MergedBea Abigail BrocalNo ratings yet
- How To Make A Nursing Care PlanDocument2 pagesHow To Make A Nursing Care PlanBea Abigail BrocalNo ratings yet
- NCP FormatDocument1 pageNCP FormatBea Abigail BrocalNo ratings yet
- NCP ExampleDocument4 pagesNCP ExampleBea Abigail BrocalNo ratings yet