You might also like
- Living with Metastatic Breast Cancer: Stories of Faith and HopeFrom EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeNo ratings yet
- Major R Cance Er Miles Stones: Overvie EwDocument14 pagesMajor R Cance Er Miles Stones: Overvie Ewtkobosz4877No ratings yet
- Breast Cancer Staging PDFDocument12 pagesBreast Cancer Staging PDFDanu BagoesNo ratings yet
- Nihms 528278Document19 pagesNihms 528278Adrian HaningNo ratings yet
- Mangacu (Cancer Journal)Document2 pagesMangacu (Cancer Journal)Diana Rose MangacuNo ratings yet
- Adjuvant Systemic Therapies in Breast CancerDocument19 pagesAdjuvant Systemic Therapies in Breast CancerSapp ChaamaraNo ratings yet
- Cytotoxic Treatment of Metastatic Breast Cancer Which Drugs and Drug Combinations To UseDocument7 pagesCytotoxic Treatment of Metastatic Breast Cancer Which Drugs and Drug Combinations To UseGamer MadaNo ratings yet
- Side Effect of Adjuvant Breast Cancer TreatmentDocument12 pagesSide Effect of Adjuvant Breast Cancer TreatmentwillyoueverlovemenkNo ratings yet
- Early Breast CancaerDocument17 pagesEarly Breast CancaerDwi Arnhilah Miranda100% (1)
- APBIDocument28 pagesAPBIWindy HardiyantyNo ratings yet
- Research Article: Prevalence of Cachexia in Cancer PatientsDocument9 pagesResearch Article: Prevalence of Cachexia in Cancer Patientsadri20121989No ratings yet
- Lubitz Et Al - The Changing Landscape of Papillary Thyroid Cancer Epidemiology, Management, and The Implications For PatientsDocument6 pagesLubitz Et Al - The Changing Landscape of Papillary Thyroid Cancer Epidemiology, Management, and The Implications For PatientsDedy AditiaNo ratings yet
- Prophylactic MastectomyDocument5 pagesProphylactic MastectomyMuhammad Darussalam DarwisNo ratings yet
- CA ServiksDocument10 pagesCA ServiksAndi Farid ANo ratings yet
- Ductal Carcinoma in Situ: How Much Is Too Much?: Keerthi Gogineni, MD, MSHPDocument3 pagesDuctal Carcinoma in Situ: How Much Is Too Much?: Keerthi Gogineni, MD, MSHPCarlos OlivoNo ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- 1-s2.0-S2352578919301018-mainDocument4 pages1-s2.0-S2352578919301018-mainmbenitezNo ratings yet
- Ovarian CancerDocument7 pagesOvarian CancerAndi AliNo ratings yet
- 007 - Clinical-Trials-That-Have-Informed-the-Modern - 2023 - Surgical-Oncology-ClinicsDocument20 pages007 - Clinical-Trials-That-Have-Informed-the-Modern - 2023 - Surgical-Oncology-ClinicsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- EBM Review Units1 4Document8 pagesEBM Review Units1 4Aissha ArifNo ratings yet
- Bristow 2002Document12 pagesBristow 2002Lưu Chính HữuNo ratings yet
- Prognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPDocument11 pagesPrognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPEndang Rahayu Fuji LestaryNo ratings yet
- Breast Imaging Methods GuideDocument22 pagesBreast Imaging Methods GuidemaytorenacgerNo ratings yet
- BiostatsDocument11 pagesBiostatsdalia khamoNo ratings yet
- Jco 1997 15 3 974Document13 pagesJco 1997 15 3 974nuriaNo ratings yet
- (Mama) Brady1977Document7 pages(Mama) Brady1977Gabriela Silva MartinsNo ratings yet
- Internal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionDocument3 pagesInternal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionmarrajoanaNo ratings yet
- Breast Cancer Treatment ThesisDocument8 pagesBreast Cancer Treatment Thesisamandamarietopeka100% (2)
- Literature Review CancerDocument7 pagesLiterature Review Cancerafdtftloi100% (1)
- 1019 5298 1 PBDocument11 pages1019 5298 1 PBm907062008No ratings yet
- Breast Cancer Treatments - Updates and New Challenges - PMCDocument75 pagesBreast Cancer Treatments - Updates and New Challenges - PMCWadood Md ZahedNo ratings yet
- Q 3 WedefDocument6 pagesQ 3 Wedefsupaidi97No ratings yet
- Analysis of Compliance, Toxicity and Survival WeeklyDocument11 pagesAnalysis of Compliance, Toxicity and Survival Weeklydanu20No ratings yet
- Will Surgery Be A Part of Breast Cancer Treatment in The FutureDocument5 pagesWill Surgery Be A Part of Breast Cancer Treatment in The FutureValentina MihaelaNo ratings yet
- Clinical Practical Guidelines in Management of Breast CancerDocument2 pagesClinical Practical Guidelines in Management of Breast CancerSittieNo ratings yet
- Hepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyDocument8 pagesHepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyGetty InasNo ratings yet
- Thesis Gastric CancerDocument4 pagesThesis Gastric Cancergj9ggjry100% (2)
- Kanker Usus BesarDocument5 pagesKanker Usus BesarwiduriwulandariNo ratings yet
- Referatneoadjuvan EnggrisDocument22 pagesReferatneoadjuvan EnggrisPonco RossoNo ratings yet
- The Clinicopathological Features and Survival Outcomes of Patients With Different Metastatic Sites in Stage IV Breast CancerDocument12 pagesThe Clinicopathological Features and Survival Outcomes of Patients With Different Metastatic Sites in Stage IV Breast CancerwidiastrikNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- Distant Breast CancerDocument10 pagesDistant Breast CancerMarion PootenNo ratings yet
- Breast Cancer Screening and Diagnosis GuideDocument261 pagesBreast Cancer Screening and Diagnosis Guidedocmaaas100% (2)
- Mcqs Mock Exams For General Surgery Board ExamDocument7 pagesMcqs Mock Exams For General Surgery Board ExamSergiu CiobanuNo ratings yet
- AJHO May17 2Document8 pagesAJHO May17 2Meiyanti MeiyantiNo ratings yet
- Does The Sequence of Anthracycline and Taxane Matter? The Neosamba TrialDocument7 pagesDoes The Sequence of Anthracycline and Taxane Matter? The Neosamba Trialyujliyur naveenNo ratings yet
- Anatomy and Breast Cancer STAGINGDocument17 pagesAnatomy and Breast Cancer STAGINGVikash SinghNo ratings yet
- Colon CancerDocument3 pagesColon CancerHeppyMeiNo ratings yet
- Chemotherapy-Induced Nausea and Vomiting in Asian Women With Breast Cancer Receiving Anthracycline-Based Adjuvant ChemotherapyDocument6 pagesChemotherapy-Induced Nausea and Vomiting in Asian Women With Breast Cancer Receiving Anthracycline-Based Adjuvant ChemotherapyMirza RisqaNo ratings yet
- PsychologicalDocument4 pagesPsychologicalDian Oktaria SafitriNo ratings yet
- Impact of Neoadjuvant Chemotherapy in Breast Cancer Patients A Single Center StudyDocument6 pagesImpact of Neoadjuvant Chemotherapy in Breast Cancer Patients A Single Center StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Whelan Et Al 2000 CancerDocument7 pagesWhelan Et Al 2000 Cancerkrishna shafiraNo ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- Management of Paget Disease of The Breast With RadiotherapyDocument8 pagesManagement of Paget Disease of The Breast With RadiotherapyAndreas RonaldNo ratings yet
- s13027 020 00299 3Document10 pagess13027 020 00299 3Remona RemoraNo ratings yet
- Epidemiologic and Socioeconomic Burden of Metastatic Renal Cell Carcinoma (MRCC) : A Literature ReviewDocument13 pagesEpidemiologic and Socioeconomic Burden of Metastatic Renal Cell Carcinoma (MRCC) : A Literature ReviewEmanuelleReisNo ratings yet
- Factors in Uencing Patient Decision-Making Between Simple Mastectomy and Surgical AlternativesDocument7 pagesFactors in Uencing Patient Decision-Making Between Simple Mastectomy and Surgical AlternativesDewi PaatNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- 10 11648 J Ejpm 20140203 11Document4 pages10 11648 J Ejpm 20140203 11intansarifnosaaNo ratings yet
- TNM ClassificationDocument18 pagesTNM ClassificationEseosa EnabuleleNo ratings yet
- Qty of Joints For FullweldingDocument1 pageQty of Joints For Fullweldingryan aniceteNo ratings yet
- How To Make AXIOM Into A ScratchpadDocument10 pagesHow To Make AXIOM Into A Scratchpadryan aniceteNo ratings yet
- JACK A Process Algebra Implementation inDocument200 pagesJACK A Process Algebra Implementation inryan aniceteNo ratings yet
- Immune Discovery May Treat All Cancer - 2020jan20Document5 pagesImmune Discovery May Treat All Cancer - 2020jan20ryan aniceteNo ratings yet
- Bisphenol A Elimination by TAML+Hydrogen Peroxide - Collins 2017Document29 pagesBisphenol A Elimination by TAML+Hydrogen Peroxide - Collins 2017ryan aniceteNo ratings yet
- Schedule 80 Clear PVC Data SheetDocument1 pageSchedule 80 Clear PVC Data Sheetryan aniceteNo ratings yet
- On The Design and Construction of AlgebrDocument11 pagesOn The Design and Construction of Algebrryan aniceteNo ratings yet
- 1.3 Schedule: Schedule Work Performed This PeriodDocument1 page1.3 Schedule: Schedule Work Performed This Periodryan aniceteNo ratings yet
- Interfacing R E D U C E To Java: and andDocument2 pagesInterfacing R E D U C E To Java: and andryan aniceteNo ratings yet
- Excel Vba-Based Solution To Pipe Flow Measurement Problem: Spreadsheets in Education (Ejsie)Document16 pagesExcel Vba-Based Solution To Pipe Flow Measurement Problem: Spreadsheets in Education (Ejsie)ryan aniceteNo ratings yet
- Symbolic Script Programming For Java: June 2009Document17 pagesSymbolic Script Programming For Java: June 2009ryan aniceteNo ratings yet
- Autocad 2D: Training ManualDocument94 pagesAutocad 2D: Training Manualryan aniceteNo ratings yet
- Designing a Digital Library of Mathematical FunctionsDocument14 pagesDesigning a Digital Library of Mathematical Functionsryan aniceteNo ratings yet
- Inside Reduce: Arthur C. Norman Raffaele VitoloDocument82 pagesInside Reduce: Arthur C. Norman Raffaele Vitoloryan aniceteNo ratings yet
- Installation Manual: System Air ConditionersDocument23 pagesInstallation Manual: System Air Conditionersryan aniceteNo ratings yet
- FXZQ-MVE DatabookDocument22 pagesFXZQ-MVE Databookryan aniceteNo ratings yet
- Cat Eye SyndromeDocument8 pagesCat Eye SyndromeBridget ColemanNo ratings yet
- Nurses Need to Know About Stroke CareDocument68 pagesNurses Need to Know About Stroke CareSuci Aning TNo ratings yet
- Staphylococcus EpidermidisDocument4 pagesStaphylococcus Epidermidisemanuel santiago triana rujanaNo ratings yet
- WA Tuberculosis Control Program BCG Vaccination GuideDocument3 pagesWA Tuberculosis Control Program BCG Vaccination GuideAdham MisdarNo ratings yet
- Idiopathic Macular HoleDocument2 pagesIdiopathic Macular Holemightyw01No ratings yet
- The Human Body: Prevention of DiseasesDocument32 pagesThe Human Body: Prevention of DiseasesbhaskarbhatiaNo ratings yet
- Incidence of Malaria Among Children Under Five in Sabuwa LGADocument43 pagesIncidence of Malaria Among Children Under Five in Sabuwa LGAUsman Ahmad TijjaniNo ratings yet
- Sexually Transmitted Infections: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine, ABUTH ZariaDocument14 pagesSexually Transmitted Infections: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine, ABUTH ZariaSalihu MustaphaNo ratings yet
- Aegypti and Aedes Albopictus. There Are Four DistinctDocument5 pagesAegypti and Aedes Albopictus. There Are Four DistinctChia Yin NgNo ratings yet
- Project PBL 4 (Chapter 13) (Activity 13.2) (M/s 258) : Name: Tee Ke Xuan Class: 4 Theta Teacher: Pn. SalmahDocument12 pagesProject PBL 4 (Chapter 13) (Activity 13.2) (M/s 258) : Name: Tee Ke Xuan Class: 4 Theta Teacher: Pn. SalmahTee KE XuanNo ratings yet
- Test Bank For Introduction To Critical Care Nursing 6th Edition Mary Lou SoleDocument8 pagesTest Bank For Introduction To Critical Care Nursing 6th Edition Mary Lou Solemammonphysics2e1.w4No ratings yet
- Causes Symptoms Diagnosis Treatment EndocarditisDocument12 pagesCauses Symptoms Diagnosis Treatment EndocarditisPriyanjali SainiNo ratings yet
- Implementing NICE Guidance on Bacterial MeningitisDocument18 pagesImplementing NICE Guidance on Bacterial MeningitisZarwo Black UstadzNo ratings yet
- Approach To A Patient With Fever?: 1 DR - Shamol /inter/feverDocument28 pagesApproach To A Patient With Fever?: 1 DR - Shamol /inter/feverkiloNo ratings yet
- Risk factors for respiratory infectionsDocument9 pagesRisk factors for respiratory infectionsGalihCandraKusumaNo ratings yet
- Volume3 Issue4 Jul Aug No.329 665 667Document3 pagesVolume3 Issue4 Jul Aug No.329 665 667MadeKurniawanAsNo ratings yet
- Leprosy Prevalence Among Nomadic Pastoralists in Northern NigeriaDocument9 pagesLeprosy Prevalence Among Nomadic Pastoralists in Northern NigeriaFredgar22No ratings yet
- Inside Reading Unit 2 Test: ©oxford University Press. Permission Granted To Reproduce For Classroom UseDocument4 pagesInside Reading Unit 2 Test: ©oxford University Press. Permission Granted To Reproduce For Classroom UsepeinisNo ratings yet
- Management of Disease Through Yoga and Nature CureDocument17 pagesManagement of Disease Through Yoga and Nature CureAnushree ChauhanNo ratings yet
- Hubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahDocument4 pagesHubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahFauzan MuttaqinNo ratings yet
- Interesting Facts About Yailin La Mas ViralijomiDocument2 pagesInteresting Facts About Yailin La Mas Viralijomiscentbeast8No ratings yet
- CARDIAC EMERGENCIES IN DAILY PRACTICEDocument45 pagesCARDIAC EMERGENCIES IN DAILY PRACTICEnikenNo ratings yet
- Volume 9 No 1Document94 pagesVolume 9 No 1ChristopherLawrenceNo ratings yet
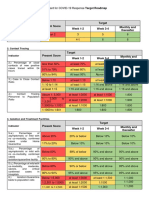
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Drug Name, Classification, Indication, Side Effects, Special Precautions, and Nursing ResponsibilitiesDocument3 pagesDrug Name, Classification, Indication, Side Effects, Special Precautions, and Nursing ResponsibilitiesPaula Suplico NiangarNo ratings yet
- Drug StudyDocument4 pagesDrug StudyForbidden fruitNo ratings yet
- NSTP QUIZ - Feb. 14, 2022 - Google FormsDocument3 pagesNSTP QUIZ - Feb. 14, 2022 - Google FormsDarlene De PazNo ratings yet
- Maritime Declaration of Health 3Document1 pageMaritime Declaration of Health 3Geoffrey AchasNo ratings yet
- Community Health NursingDocument2 pagesCommunity Health NursingKevin WangokhoNo ratings yet
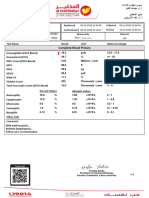
- Tests Results 66423514212Document2 pagesTests Results 66423514212ramadan.seydNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet