You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ms Rebecca General Communication SkillDocument44 pagesMs Rebecca General Communication Skilliq_dianaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Klarkowski 2013Document14 pagesKlarkowski 2013iq_dianaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- DR Gabriel Wallau Genomic Data Sharing Covid19 BrazilDocument18 pagesDR Gabriel Wallau Genomic Data Sharing Covid19 Braziliq_dianaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- DR Oliver Morgan International Pathogen Surveillance NetoworkDocument16 pagesDR Oliver Morgan International Pathogen Surveillance Netoworkiq_dianaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Molecular Template MfrsDocument41 pagesMolecular Template Mfrsiq_dianaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- MR Tapiwanashe Training Nasal Antigen ZimbabweDocument25 pagesMR Tapiwanashe Training Nasal Antigen Zimbabweiq_dianaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- King 1994Document6 pagesKing 1994iq_dianaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MR Solomon Training Antigen SomaliaDocument10 pagesMR Solomon Training Antigen Somaliaiq_dianaNo ratings yet
- COVID-19 Testing One Size Does Not Fit AllDocument3 pagesCOVID-19 Testing One Size Does Not Fit Alliq_dianaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- COVID19 Specimen Acceptability - LDT Roche Revised Version v4 32020Document11 pagesCOVID19 Specimen Acceptability - LDT Roche Revised Version v4 32020iq_dianaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- DR Jilian WHO Webinar Covid Self Testing GuideDocument10 pagesDR Jilian WHO Webinar Covid Self Testing Guideiq_dianaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Materi DR Thyrza - Qualified DBS For Newborn Screening Test RevDocument60 pagesMateri DR Thyrza - Qualified DBS For Newborn Screening Test Reviq_dianaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DR Lara Vojnov Severe Acute Hepatitis of Unknown Aetiology WHO Incident Team Who WebinarDocument14 pagesDR Lara Vojnov Severe Acute Hepatitis of Unknown Aetiology WHO Incident Team Who Webinariq_dianaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- BiochemMed2019 01Document6 pagesBiochemMed2019 01iq_dianaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- COVID-19 Back Tie Don Doff ChecklistDocument2 pagesCOVID-19 Back Tie Don Doff Checklistiq_dianaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 22 02 02 WHO EUL - PHLabs US Final - DR Ute FinalDocument10 pages22 02 02 WHO EUL - PHLabs US Final - DR Ute Finaliq_dianaNo ratings yet
- Dr. Ni Made Hustrini, SPPD-KGH - CKD Sysmex - 280522Document33 pagesDr. Ni Made Hustrini, SPPD-KGH - CKD Sysmex - 280522iq_dianaNo ratings yet
- One-Step Real-Time RT-PCR Test For COVID-19Document3 pagesOne-Step Real-Time RT-PCR Test For COVID-19iq_dianaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Dr. Weny Rinawati - Important and Novel Biomarker For HepatitisDocument24 pagesDr. Weny Rinawati - Important and Novel Biomarker For Hepatitisiq_dianaNo ratings yet
- Ichroma HbA1C1Document1 pageIchroma HbA1C1iq_dianaNo ratings yet
- Activities Booklet - EN - GenCommDocument3 pagesActivities Booklet - EN - GenCommiq_dianaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Contribution Statistical Evaluation Data For External Quality AssessmentDocument248 pagesContribution Statistical Evaluation Data For External Quality Assessmentiq_dianaNo ratings yet
- Index in Platelet Aggregation Analysis Fea and Effect Antiplatelet TherapiesDocument9 pagesIndex in Platelet Aggregation Analysis Fea and Effect Antiplatelet Therapiesiq_dianaNo ratings yet
- Impact of Environmental Design On Doffing Personal Protective Equipment in A Healthcare Environment A Formative Human Factors TrialDocument7 pagesImpact of Environmental Design On Doffing Personal Protective Equipment in A Healthcare Environment A Formative Human Factors Trialiq_dianaNo ratings yet
- HSE Covid-19 Doffing CoverallDocument1 pageHSE Covid-19 Doffing Coveralliq_dianaNo ratings yet
- Phytopathogenic Fungi With Potential As Biocontrol Agents For Weeds of Importance in Crops of Antioquia, ColombiaDocument15 pagesPhytopathogenic Fungi With Potential As Biocontrol Agents For Weeds of Importance in Crops of Antioquia, ColombiaFabian GarzonNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Reconstruction of The Lineage Y Chromosome HaplotypeDocument13 pagesReconstruction of The Lineage Y Chromosome HaplotypeЛалю МетевNo ratings yet
- Organisms and Population Flowchart - Telegram Ishita 4 UDocument11 pagesOrganisms and Population Flowchart - Telegram Ishita 4 Ulakshya singhalNo ratings yet
- Plant and Mammalian Cell Technology (BSB 3163)Document25 pagesPlant and Mammalian Cell Technology (BSB 3163)Anis FatehahNo ratings yet
- Herosis Breeding (DR Wilson)Document8 pagesHerosis Breeding (DR Wilson)Rahul ChandraNo ratings yet
- Biology TCC Research PaperDocument4 pagesBiology TCC Research Papereugene plangananNo ratings yet
- Anthony 2021 Migration Nomads From The eDocument26 pagesAnthony 2021 Migration Nomads From The eRenan Falcheti PeixotoNo ratings yet
- Embryology and Malformation of The Female Genital Tract: Kindu YDocument37 pagesEmbryology and Malformation of The Female Genital Tract: Kindu YCHALIE MEQUNo ratings yet
- 4 AnaDocument22 pages4 Anairis casalaNo ratings yet
- DNA LibraryDocument73 pagesDNA LibraryDGA GAMINGNo ratings yet
- Primary Immunodeficiency DiseasesDocument20 pagesPrimary Immunodeficiency Diseasesodhiambo samwelNo ratings yet
- Ns Elec 4 - Muscular SystemDocument5 pagesNs Elec 4 - Muscular SystemONGLENGCO WILSON JAKE V.No ratings yet
- NeurophysiologyDocument200 pagesNeurophysiologyashley nicholeNo ratings yet
- YVEX8d587jbMbhWKb4DW 230519 232428Document7 pagesYVEX8d587jbMbhWKb4DW 230519 232428ry364970No ratings yet
- Biotechnology Safety Law enDocument40 pagesBiotechnology Safety Law enSunnyNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Botany Major Syllabus For U.G. (Session 2021-22) 183Document53 pagesBotany Major Syllabus For U.G. (Session 2021-22) 183Kaushikee KatyayaniNo ratings yet
- CM1-CU3 - CellsDocument15 pagesCM1-CU3 - CellsKat JornadalNo ratings yet
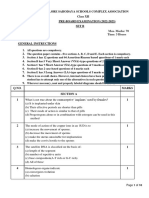
- CLASSXIIPreboardBIOLOGY-SET2QuestionPaper 97387Document10 pagesCLASSXIIPreboardBIOLOGY-SET2QuestionPaper 97387worksmartvaishNo ratings yet
- Bok:978 3 642 37922 2Document615 pagesBok:978 3 642 37922 2atilio martinezNo ratings yet
- NucleotidesDocument12 pagesNucleotidesIlac Tristan BernardoNo ratings yet
- ClinPara AmoebaDocument8 pagesClinPara AmoebaStephen YorNo ratings yet
- Kuliah Jamur Genetika 2014Document22 pagesKuliah Jamur Genetika 2014Maskur Fahmi ÄdibasNo ratings yet
- Sci and Tech Pre PyqDocument37 pagesSci and Tech Pre PyqNishant RajNo ratings yet
- Oeq 2Document7 pagesOeq 2Sara JosephNo ratings yet
- Sumber GambarDocument3 pagesSumber GambarsuryaningsihNo ratings yet
- Grade 11 Life Sciences Revision Material Term 1 2023Document30 pagesGrade 11 Life Sciences Revision Material Term 1 2023Junior NgwenyaNo ratings yet
- Morphosolation Characteristic of The Flower of Liliaceae Rare Species of The Namangan Region of The Areal DistributionDocument6 pagesMorphosolation Characteristic of The Flower of Liliaceae Rare Species of The Namangan Region of The Areal DistributionresearchparksNo ratings yet
- The MOR (Mu Opioid Receptor) and FLNA (Filamin A)Document28 pagesThe MOR (Mu Opioid Receptor) and FLNA (Filamin A)lara gay villaruzNo ratings yet
- Intracellular Compartments and Transport Cytoskeleton-1Document32 pagesIntracellular Compartments and Transport Cytoskeleton-1Sohan rautNo ratings yet
- 1/ Giới Thiệu: 1.1 Thuyết tiến hóaDocument36 pages1/ Giới Thiệu: 1.1 Thuyết tiến hóaNgô Thị Thắng LợiNo ratings yet
- All That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesFrom EverandAll That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesRating: 4.5 out of 5 stars4.5/5 (397)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (393)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceFrom EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceRating: 4.5 out of 5 stars4.5/5 (517)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)