You might also like
- Clinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementDocument24 pagesClinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementSubhashish DasNo ratings yet
- NEJMcpc 2312731Document11 pagesNEJMcpc 2312731cehborrotoNo ratings yet
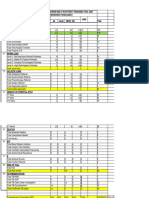
- Medical Unit-November Wk3 - Summary IndicatorsDocument9 pagesMedical Unit-November Wk3 - Summary IndicatorsGeorge ApaNo ratings yet
- Icu Clinical Audit of Month of April 2021 G.C: Prepared By:dr Nigat Endalamaw Emccr2 Moderator:Dr AyalewDocument57 pagesIcu Clinical Audit of Month of April 2021 G.C: Prepared By:dr Nigat Endalamaw Emccr2 Moderator:Dr AyalewalexNo ratings yet
- St. Peter's Hospital Reviews TB Treatment ProgramDocument43 pagesSt. Peter's Hospital Reviews TB Treatment Programሀይደር ዶ.ርNo ratings yet
- Pericarditis in Rheumatoid ArthritisDocument4 pagesPericarditis in Rheumatoid ArthritisIJAR JOURNALNo ratings yet
- Title: To Assess Predictors For Platelet Transfusion in Tropical Viral Fever WithDocument8 pagesTitle: To Assess Predictors For Platelet Transfusion in Tropical Viral Fever WithNarendra PatilNo ratings yet
- Urinalysis Parameters For Predicting Severity in COVIDDocument3 pagesUrinalysis Parameters For Predicting Severity in COVIDTania MNo ratings yet
- Introduction To Biostatistics DR Sahar KhashabDocument161 pagesIntroduction To Biostatistics DR Sahar Khashabnada9tarek-2No ratings yet
- Acute Kidney FailureDocument8 pagesAcute Kidney FailureJuan Diego Ferreyros ArroyoNo ratings yet
- Report COVID Clinical ManagmentDocument70 pagesReport COVID Clinical ManagmentJeevan Emmanual JoyNo ratings yet
- Evaluation of Platelet Count and Platelet Indices in Covid-19 InfectionDocument6 pagesEvaluation of Platelet Count and Platelet Indices in Covid-19 InfectionIJAR JOURNALNo ratings yet
- Appendix StudyDocument5 pagesAppendix StudySunil RevankarNo ratings yet
- Liaison Services in General HospitalsDocument41 pagesLiaison Services in General HospitalsrowanpurdyNo ratings yet
- Bharati U PDFDocument4 pagesBharati U PDFAnish ShresthaNo ratings yet
- Ma DPH Covid-19 DashboardDocument14 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- Hematologic Parameters in Patients With COVID-19 InfectionDocument4 pagesHematologic Parameters in Patients With COVID-19 InfectionLuisa María EstrellaNo ratings yet
- Ma DPH Covid-19 DashboardDocument16 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- Erj 02096 2020Document4 pagesErj 02096 2020Alexandra IonițăNo ratings yet
- Relationship between hemodialysis duration, comorbid factors and mortality in chronic kidney failure patientsDocument6 pagesRelationship between hemodialysis duration, comorbid factors and mortality in chronic kidney failure patients201801083 RosantiNo ratings yet
- Invasive Mechanical Ventilation in COVID-19 Patient Management: The Experience With 469 Patients in WuhanDocument3 pagesInvasive Mechanical Ventilation in COVID-19 Patient Management: The Experience With 469 Patients in WuhanGeysel SuarezNo ratings yet
- Huntsville Hospital System COVID-19 Statistics As of Sept. 1Document3 pagesHuntsville Hospital System COVID-19 Statistics As of Sept. 1FOX54 News HuntsvilleNo ratings yet
- Validation of Severity Scoring Systems SAPS II and APACHE II in A Single-Center PopulationDocument7 pagesValidation of Severity Scoring Systems SAPS II and APACHE II in A Single-Center Populationteguh sNo ratings yet
- E1172 FullDocument8 pagesE1172 FullZairenee QuizanaNo ratings yet
- Herniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung IndonesiaDocument7 pagesHerniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung Indonesiawulan dwi yulistiaNo ratings yet
- JTH 14848Document10 pagesJTH 14848Ayesha IkhlaqNo ratings yet
- 411 1828 1 PB PDFDocument5 pages411 1828 1 PB PDFednihsNo ratings yet
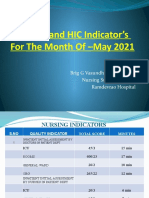
- Nursing and HIC Indicator's For The Month of - May 2021Document9 pagesNursing and HIC Indicator's For The Month of - May 2021Kamalakar KaramchetiNo ratings yet
- Huntsville Hospital Health System: Day-by-Day # of COVID-19 InpatientsDocument3 pagesHuntsville Hospital Health System: Day-by-Day # of COVID-19 Inpatientskovi mNo ratings yet
- Ma DPH Covid-19 DashboardDocument16 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- Platelet transfusions in dengue may not reduce bleedingDocument6 pagesPlatelet transfusions in dengue may not reduce bleedingtiara_nienNo ratings yet
- dbv27p138 PDFDocument6 pagesdbv27p138 PDFElizabeth Puji YantiNo ratings yet
- It S Time To Stop Talking About Delayed Transfers of CareDocument9 pagesIt S Time To Stop Talking About Delayed Transfers of CarePhuong AnhNo ratings yet
- Alvarado scoring accurately diagnoses appendicitisDocument5 pagesAlvarado scoring accurately diagnoses appendicitisMahlina Nur LailiNo ratings yet
- Patient Covid-19 Test Results and Clinical NotesDocument2 pagesPatient Covid-19 Test Results and Clinical NotesayushNo ratings yet
- OSDH COVID-19 Report 4-21-2020Document16 pagesOSDH COVID-19 Report 4-21-2020KFORNo ratings yet
- Ma DPH Covid-19 DashboardDocument16 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- Supplementary Online Content: © 2020 American Medical Association. All Rights ReservedDocument19 pagesSupplementary Online Content: © 2020 American Medical Association. All Rights ReservedMai GonzalezNo ratings yet
- Ma DPH Covid-19 DashboardDocument16 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- 2015-01-01 Norms For The Health Cadre - Sri LankaDocument83 pages2015-01-01 Norms For The Health Cadre - Sri LankaDoctors News86% (7)
- Case 3-2020: A 44-Year-Old Man With Weight Loss, Diarrhea, and Abdominal PainDocument10 pagesCase 3-2020: A 44-Year-Old Man With Weight Loss, Diarrhea, and Abdominal PainAlvaro Andres Flores JimenezNo ratings yet
- 2011ooPediatricHandbook PDFDocument146 pages2011ooPediatricHandbook PDFSven OrdanzaNo ratings yet
- Laboratory Abnormalities in Patients with COVID-19Document4 pagesLaboratory Abnormalities in Patients with COVID-19Angelica Ferrer TrujequeNo ratings yet
- Ojmm 2016031815244658Document6 pagesOjmm 2016031815244658Mohamed KadleNo ratings yet
- Using VA Nursing Data To Estimate The Relationship Between Nurse Staffing and Patient OutcomesDocument28 pagesUsing VA Nursing Data To Estimate The Relationship Between Nurse Staffing and Patient OutcomesTarandam INo ratings yet
- Data Code DescriptionDocument8 pagesData Code DescriptionAyushi JainNo ratings yet
- RDW Levels Associated With Venous Thrombosis RiskDocument6 pagesRDW Levels Associated With Venous Thrombosis RiskJicko Street HooligansNo ratings yet
- WD 3D November WK 4tracking ToolDocument24 pagesWD 3D November WK 4tracking ToolGeorge ApaNo ratings yet
- Presumed Asymptomatic Carrier Transmission of COVID-19Document2 pagesPresumed Asymptomatic Carrier Transmission of COVID-19SarrrrrrrNo ratings yet
- Ma DPH Covid-19 DashboardDocument14 pagesMa DPH Covid-19 DashboardJohn WallerNo ratings yet
- Lab Literacy for Doctors: A Guide to Ordering the Right Tests for Better Patient CareFrom EverandLab Literacy for Doctors: A Guide to Ordering the Right Tests for Better Patient CareRating: 3.5 out of 5 stars3.5/5 (3)
- NICE Way to Cure COVID -19From EverandNICE Way to Cure COVID -19Rating: 4.5 out of 5 stars4.5/5 (8)
- Old and Sick in America: The Journey through the Health Care SystemFrom EverandOld and Sick in America: The Journey through the Health Care SystemNo ratings yet
- Unveiling the Secrets of Laboratories: The Importance of Clinical Analysisin Health and Disease DiagnosFrom EverandUnveiling the Secrets of Laboratories: The Importance of Clinical Analysisin Health and Disease DiagnosNo ratings yet
- Laboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceFrom EverandLaboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceRating: 5 out of 5 stars5/5 (3)
- Ventricular-Assist Devices and Kidney Disease: Clinical PerspectivesFrom EverandVentricular-Assist Devices and Kidney Disease: Clinical PerspectivesChaitanya DesaiNo ratings yet
- Head and Neck Cancer Care in a Pandemic: Prioritizing Safe CareFrom EverandHead and Neck Cancer Care in a Pandemic: Prioritizing Safe CareNo ratings yet
- The Vatican As A World Power (1939)Document481 pagesThe Vatican As A World Power (1939)sexylove1477No ratings yet
- Train LapbookDocument34 pagesTrain LapbookSebõk KatalinNo ratings yet
- Argacel TCW_enDocument2 pagesArgacel TCW_enUtpalNo ratings yet
- Underwater vessels, sensors, weapons and control systemsDocument1 pageUnderwater vessels, sensors, weapons and control systemsNguyễn ThaoNo ratings yet
- Elah'Im CultureDocument60 pagesElah'Im CultureRichard David DellermanNo ratings yet
- Presentation On Indian Railways-03Document18 pagesPresentation On Indian Railways-03Shweta SinghNo ratings yet
- X1jet MX Manual PDFDocument97 pagesX1jet MX Manual PDFrithik srivastavaNo ratings yet
- Roke TsanDocument53 pagesRoke Tsanhittaf_05No ratings yet
- Early strength predicts long-term performance of asphalt cold mixesDocument7 pagesEarly strength predicts long-term performance of asphalt cold mixesMonu GhadwalNo ratings yet
- HBR - Michael Porter - Redefining Competition in Healthcare - 2004 PDFDocument14 pagesHBR - Michael Porter - Redefining Competition in Healthcare - 2004 PDFYusfin DelfitaNo ratings yet
- LMV Tyre SafetyDocument19 pagesLMV Tyre SafetykarvadNo ratings yet
- Typical Specification of Volvo Truck PDFDocument3 pagesTypical Specification of Volvo Truck PDFKartik BehereNo ratings yet
- Samantha Serpas ResumeDocument1 pageSamantha Serpas Resumeapi-247085580No ratings yet
- Creative 2nd QuarterDocument6 pagesCreative 2nd QuarterJanice CordovaNo ratings yet
- German UnificationDocument40 pagesGerman UnificationJosephlangeloNo ratings yet
- Inventions Crossword PuzzleDocument2 pagesInventions Crossword PuzzleAimri910% (1)
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Document2 pagesRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriNo ratings yet
- Helmut Lethen - Cool Conduct - The Culture of Distance in Weimar Germany (Weimar and Now - German Cultural Criticism) - University of California Press (2001) PDFDocument265 pagesHelmut Lethen - Cool Conduct - The Culture of Distance in Weimar Germany (Weimar and Now - German Cultural Criticism) - University of California Press (2001) PDFJaco CMNo ratings yet
- The Impact of Interest Rates On Economic Growth in KenyaDocument41 pagesThe Impact of Interest Rates On Economic Growth in KenyaSAMUEL KIMANINo ratings yet
- Valplast: Flexible, Esthetic Partial DenturesDocument4 pagesValplast: Flexible, Esthetic Partial Denturesአነኬ ቹህቺዶሃሠኪቺጆቺNo ratings yet
- Drewry Capability StatementDocument9 pagesDrewry Capability Statementmanis_sgsNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- Wind Energy Services Brochure 4696 3 Da en PDFDocument62 pagesWind Energy Services Brochure 4696 3 Da en PDFghadasaudiNo ratings yet
- Macalloy Corporate Brochure September 2018 LR PDFDocument12 pagesMacalloy Corporate Brochure September 2018 LR PDFsampathkumarNo ratings yet
- Dodigen 2808 TDSDocument1 pageDodigen 2808 TDSRashid SaleemNo ratings yet
- ACHD 07 The Innsmouth ConspiracyDocument6 pagesACHD 07 The Innsmouth ConspiracyJNo ratings yet
- Vehicle Speed Control Using RF CommunicationDocument20 pagesVehicle Speed Control Using RF CommunicationRaina John100% (2)
- Hexadecimal Numbers ExplainedDocument51 pagesHexadecimal Numbers Explainedmike simsonNo ratings yet
- Sample Final Exam Larkin AnswersDocument18 pagesSample Final Exam Larkin AnswersLovejot SinghNo ratings yet
- Congress Vienna QuestionsDocument5 pagesCongress Vienna QuestionsElliott CookNo ratings yet