You might also like
- 2019 SEATTLE CHILDREN'S Hospital. Healthcare-Professionals:clinical-Standard-Work-Asthma - PathwayDocument41 pages2019 SEATTLE CHILDREN'S Hospital. Healthcare-Professionals:clinical-Standard-Work-Asthma - PathwayVladimir Basurto100% (1)
- Pulmonology Step2 CKDocument22 pagesPulmonology Step2 CKsarwat86% (7)
- GINA (Asma) 2022-20-45Document26 pagesGINA (Asma) 2022-20-45Rianda AkmalNo ratings yet
- GINA Main Report 2022 21 43Document23 pagesGINA Main Report 2022 21 43Daniela BecerraNo ratings yet
- The Asthma-COPD Overlap Syndrome: LT Col John F. Freiler, MDDocument5 pagesThe Asthma-COPD Overlap Syndrome: LT Col John F. Freiler, MDIan HuangNo ratings yet
- ACOSDocument6 pagesACOSVamsi krishna GaddeNo ratings yet
- Asthma-COPD Overlap Syndrome (ACOS) : Is It A Common Entity?Document36 pagesAsthma-COPD Overlap Syndrome (ACOS) : Is It A Common Entity?Linto JohnNo ratings yet
- Gold 2023 (016 193)Document178 pagesGold 2023 (016 193)Mariana Tovar RodriguezNo ratings yet
- Asthma-COPD Overlap: EditorialDocument2 pagesAsthma-COPD Overlap: EditorialAfifah RizkianaNo ratings yet
- Asthma, COPD and Asthma-COPD Overlap Syndrome (GINA 2014)Document16 pagesAsthma, COPD and Asthma-COPD Overlap Syndrome (GINA 2014)dinh son myNo ratings yet
- Asthma Copd OverlapDocument16 pagesAsthma Copd OverlapMaryam BurhanuddinNo ratings yet
- ACOSDocument14 pagesACOSDejan ŽujovićNo ratings yet
- 4 6048890192880730833Document332 pages4 6048890192880730833Rin4lNo ratings yet
- Asthma-COPD Overlap SyndromeDocument38 pagesAsthma-COPD Overlap SyndromeSanjay NavaleNo ratings yet
- Imaging in Chronic Obstructive Pulmonary DiseaseDocument9 pagesImaging in Chronic Obstructive Pulmonary DiseasePramusetya SuryandaruNo ratings yet
- Natural History and Mechanisms of COPD: Invited Review Series: Copd: New HorizonsDocument24 pagesNatural History and Mechanisms of COPD: Invited Review Series: Copd: New HorizonsSebastian RamirezNo ratings yet
- Pulmonary Overlap Syndromes, With A Focus On COPD and ILDDocument15 pagesPulmonary Overlap Syndromes, With A Focus On COPD and ILDsavvy_as_98-1No ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Diagnosis and ManagementDocument19 pagesChronic Obstructive Pulmonary Disease (COPD) : Diagnosis and ManagementtiaranindyNo ratings yet
- COPD AsthmaDocument12 pagesCOPD AsthmaShuey ChinNo ratings yet
- Imaging in Chronic Obstructive Pulmonary DiseaseDocument9 pagesImaging in Chronic Obstructive Pulmonary DiseaseHarizNo ratings yet
- Unravelling Young COPD and Pre-COPD in The General PopulationDocument11 pagesUnravelling Young COPD and Pre-COPD in The General PopulationLorena ZirondiNo ratings yet
- Management Acute ExacerbationDocument4 pagesManagement Acute ExacerbationAmalia Nurul UlumNo ratings yet
- Copd PDFDocument28 pagesCopd PDFDarawan MirzaNo ratings yet
- Nur 111 Session 1 Sas 1Document8 pagesNur 111 Session 1 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- CopdDocument3 pagesCopdFawad HameediNo ratings yet
- GOLD PocketGuide 2011 Jan18Document32 pagesGOLD PocketGuide 2011 Jan18Teresa ChangNo ratings yet
- Hamad 2020Document3 pagesHamad 2020Ella EllaNo ratings yet
- 2019 - Chronic Obstructive Pulmonary Disease andDocument6 pages2019 - Chronic Obstructive Pulmonary Disease andAndreea MoalesNo ratings yet
- NCMB 312 M1 Cu3Document16 pagesNCMB 312 M1 Cu3Georgia De OcampoNo ratings yet
- NCMB312M1CU3Document16 pagesNCMB312M1CU3Georgia De OcampoNo ratings yet
- Copd: Defining and Magnitude of ProblemDocument37 pagesCopd: Defining and Magnitude of ProblemSiti AmandaNo ratings yet
- Obstructive Pulmonary DiseasesDocument42 pagesObstructive Pulmonary Diseasesbessan alfqeatNo ratings yet
- Final DraftDocument6 pagesFinal DraftSimon KingNo ratings yet
- 418-M1-Cu 5 Resp. Emergencies 2Document12 pages418-M1-Cu 5 Resp. Emergencies 2Paradillo Regatuna LesterNo ratings yet
- Dr. Arto - ASMA PPOK COUGH CONFRENCE DV MEDAN 2019 (Edited)Document74 pagesDr. Arto - ASMA PPOK COUGH CONFRENCE DV MEDAN 2019 (Edited)Janetty TjandraNo ratings yet
- Pauwels 2004Document8 pagesPauwels 2004srichakadharsri911No ratings yet
- SalmeterolDocument10 pagesSalmeterolArezoo JamNo ratings yet
- Update in Airway Obstuction DiseaseDocument42 pagesUpdate in Airway Obstuction DiseaseTiyaTyraSidoraNo ratings yet
- Clinical Approach To The Therapy of Asthma-COPD Overlap: Recent Advances in Chest MedicineDocument10 pagesClinical Approach To The Therapy of Asthma-COPD Overlap: Recent Advances in Chest MedicinetodongtoanNo ratings yet
- Uip and NsipDocument38 pagesUip and NsipReem AbbasNo ratings yet
- Slide Kuliah PPOK 2018Document44 pagesSlide Kuliah PPOK 2018Rachma DyraNo ratings yet
- 2° Artículo de EpocDocument10 pages2° Artículo de EpocveroarujogonzalesNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Patient EducationDocument2 pagesChronic Obstructive Pulmonary Disease (COPD) : Patient EducationtiaranindyNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFEbenezer UdeNo ratings yet
- Chronic Obstructive Pulmonary Disease Diagnosis and StagingDocument50 pagesChronic Obstructive Pulmonary Disease Diagnosis and StagingSensing NonsenseNo ratings yet
- Risk Factor Nle SpiroDocument15 pagesRisk Factor Nle SpiroElla EllaNo ratings yet
- Smoking Associated Interstitial Lung Disease: Update and ReviewDocument28 pagesSmoking Associated Interstitial Lung Disease: Update and ReviewmikelNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap 2Document15 pagesGina Main Report 2022 Final 22-07-01 Wms Cap 2Lucero MalarínNo ratings yet
- Practice EamDocument35 pagesPractice EamMYKRISTIE JHO MENDEZNo ratings yet
- Anaesthesia and CopdDocument7 pagesAnaesthesia and CopdAshish PandeyNo ratings yet
- CopdDocument11 pagesCopdpkm bungamasNo ratings yet
- Abnormal Lung Physiology Through Spirometry: A Comprehensive Overview of COPDDocument12 pagesAbnormal Lung Physiology Through Spirometry: A Comprehensive Overview of COPDK.Sathvik. AcharyaNo ratings yet
- Sheet 2-COPD, 20231Document28 pagesSheet 2-COPD, 20231leensaeed26No ratings yet
- CopdDocument41 pagesCopdneelumshaukatNo ratings yet
- Chronic Obstructive Pulmonary Disease: Martina S., Selda S., Sarah A.G., Dina H., Sonia C. UMFT Victor Babes'Document39 pagesChronic Obstructive Pulmonary Disease: Martina S., Selda S., Sarah A.G., Dina H., Sonia C. UMFT Victor Babes'Petcu FlorinaNo ratings yet
- COPDDocument3 pagesCOPDdidaryadgar099No ratings yet
- Primary Care of The Patient With Chronic Obstructive Pulmonary Disease in ItalyDocument7 pagesPrimary Care of The Patient With Chronic Obstructive Pulmonary Disease in ItalyAtika Indah SariNo ratings yet
- 1.5A Copd: OutlineDocument12 pages1.5A Copd: OutlineCecille Ann Cayetano100% (1)
- Asthma: Symptoms, Treatments, and Medication for Asthma and BronchitisFrom EverandAsthma: Symptoms, Treatments, and Medication for Asthma and BronchitisNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap 6Document24 pagesGina Main Report 2022 Final 22-07-01 Wms Cap 6Lucero MalarínNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap 3Document62 pagesGina Main Report 2022 Final 22-07-01 Wms Cap 3Lucero MalarínNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap4Document17 pagesGina Main Report 2022 Final 22-07-01 Wms Cap4Lucero MalarínNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap 2Document15 pagesGina Main Report 2022 Final 22-07-01 Wms Cap 2Lucero MalarínNo ratings yet
- Gina Main Report 2022 Final 22-07-01 Wms Cap 1Document31 pagesGina Main Report 2022 Final 22-07-01 Wms Cap 1Lucero MalarínNo ratings yet
- AGUA CORPORAL TOTAL FormulasDocument5 pagesAGUA CORPORAL TOTAL FormulasLucero MalarínNo ratings yet
- Trans Pulmopatho ColoredDocument8 pagesTrans Pulmopatho Colored2012No ratings yet
- Diagnosa SeptDocument839 pagesDiagnosa Septsusi herawatiNo ratings yet
- Luaab Bahi-Dana (Mucilage) Quince SeedsDocument3 pagesLuaab Bahi-Dana (Mucilage) Quince Seedsintikhabansari100% (1)
- Budesonide FormoterolDocument2 pagesBudesonide FormoterolDeathDefying DonutNo ratings yet
- Influenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionDocument3 pagesInfluenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionYusuf Rony LosongNo ratings yet
- Aproach in Difficult Airway ManagementDocument24 pagesAproach in Difficult Airway Managementarnawa ekaNo ratings yet
- Pulm Board ReviewDocument19 pagesPulm Board ReviewAli LaftaNo ratings yet
- Covid Signs and SymptomsDocument2 pagesCovid Signs and SymptomsCarl MendozaNo ratings yet
- Assessment of Respiratory SystemDocument18 pagesAssessment of Respiratory SystemIbi Yulia Setyani100% (1)
- Bronchiolitis Seminar.Document15 pagesBronchiolitis Seminar.Sudha YadavNo ratings yet
- 03 RSV Adults Friedland 508Document23 pages03 RSV Adults Friedland 508incinerate81No ratings yet
- Free Sample Informative SpeechDocument1 pageFree Sample Informative SpeechSari Adnin HalimNo ratings yet
- 03 Diagnostic Approach To Cough PDFDocument1 page03 Diagnostic Approach To Cough PDFSindujaNo ratings yet
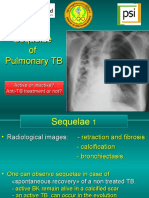
- 15c TB SequelaeDocument49 pages15c TB SequelaeWin Sein Myint100% (1)
- NCP For LEC Act. 5Document1 pageNCP For LEC Act. 5Keneth Dave AglibutNo ratings yet
- Disorder of Respiratory SystemDocument89 pagesDisorder of Respiratory SystemDarine Nasr100% (1)
- Asthma Action PlanDocument2 pagesAsthma Action PlanQuan DinhNo ratings yet
- FFFFFFF: Health Declaration Form Health Declaration Form Health Declaration FormDocument1 pageFFFFFFF: Health Declaration Form Health Declaration Form Health Declaration FormLeny Goyo LaurenteNo ratings yet
- Swine Flu PresentationDocument20 pagesSwine Flu PresentationyusufNo ratings yet
- Cough: - Atheer AljthalinDocument15 pagesCough: - Atheer AljthalinAmira AlmutairiNo ratings yet
- Nursing Care of The Child With Respiratory DysfunctionDocument54 pagesNursing Care of The Child With Respiratory DysfunctionAlexis Coronado100% (1)
- Ari WhoDocument55 pagesAri WholingghezhiNo ratings yet
- Cough Suppression v2Document2 pagesCough Suppression v2Alain CésarNo ratings yet
- Pediatric Asthma TBL QuestionsDocument4 pagesPediatric Asthma TBL QuestionsVladimir BasurtoNo ratings yet
- 16732-Article Text-75540-82300-10-20230101Document11 pages16732-Article Text-75540-82300-10-20230101Oksana VedorikaNo ratings yet
- Laporan-Diagnosa Januari 2021Document231 pagesLaporan-Diagnosa Januari 2021Putri AnnisaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument4 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsNag Sai NarahariNo ratings yet
- Occupational Lung DiseaseDocument24 pagesOccupational Lung DiseaseprachitiNo ratings yet
- A Budget of Dumb Asses 2011Document2 pagesA Budget of Dumb Asses 2011piano1985No ratings yet