You might also like
- Increasing The Elimination of Toxins in The BodyDocument33 pagesIncreasing The Elimination of Toxins in The BodyhllbakriNo ratings yet
- Chapter 2 - C - III Portal HypertensionDocument37 pagesChapter 2 - C - III Portal HypertensionEmmaNo ratings yet
- Treatment Guidelines for Poisoning and Drug OverdoseDocument19 pagesTreatment Guidelines for Poisoning and Drug Overdosemeryati sinambelaNo ratings yet
- SimulationDocument5 pagesSimulationJessFriend100% (1)
- Hemodialysis and Peritoneal DialysisDocument57 pagesHemodialysis and Peritoneal Dialysisirene joy91% (11)
- Pharmacology of Diuretics: DR - Datten Bangun MSC, SPFKDocument46 pagesPharmacology of Diuretics: DR - Datten Bangun MSC, SPFKRizky Pramata Simamora 19000029No ratings yet
- DiureticsDocument29 pagesDiureticsdeepak askarNo ratings yet
- F. Fluids, Electrolytes Renal ManagementDocument45 pagesF. Fluids, Electrolytes Renal Managementcoco brillqnteNo ratings yet
- Renal Replacement Therapies: Hemodialysis and Peritoneal DialysisDocument86 pagesRenal Replacement Therapies: Hemodialysis and Peritoneal DialysisSabita Tripathi100% (2)
- Dialysis 200819075444Document96 pagesDialysis 200819075444nadeeshashami675No ratings yet
- 4 General Pharmacology AliexcretionDocument31 pages4 General Pharmacology AliexcretionAurelia DS SequeiraNo ratings yet
- Dialysis Applications in Biomedical and Chemical IndustriesDocument23 pagesDialysis Applications in Biomedical and Chemical IndustriesRaviIdhayachanderNo ratings yet
- DIALYSISDocument6 pagesDIALYSISJobelle AcenaNo ratings yet
- DIALYSIS ProcedureDocument8 pagesDIALYSIS ProcedureRaman SamraoNo ratings yet
- Envenomation and IntoxicationDocument37 pagesEnvenomation and IntoxicationYoelBagusGiartoNo ratings yet
- Functions of The KidneyDocument7 pagesFunctions of The KidneyKOFI BROWNNo ratings yet
- Definition-Acute Kidney InjuryDocument6 pagesDefinition-Acute Kidney Injuryashi leginNo ratings yet
- Extra Corporeal Removal of DrugsDocument25 pagesExtra Corporeal Removal of Drugsyuppie_raj2175No ratings yet
- Drugs Affecting Renal SystemDocument58 pagesDrugs Affecting Renal SystemDaniel OkakaNo ratings yet
- CRRTDocument61 pagesCRRTArdeleanu Costin100% (1)
- NCLEX UrinaryDocument35 pagesNCLEX UrinaryAnonymous 1EoKWlNo ratings yet
- DIALYSIS ReportingDocument10 pagesDIALYSIS ReportingGlenelyn Grace InfanteNo ratings yet
- Drugs Therapy For Kidney: Budi RaharjoDocument33 pagesDrugs Therapy For Kidney: Budi RaharjoNurul MasyithahNo ratings yet
- Hemodialysi S: Ariane Jake C. Fernandez, RN, MSNDocument37 pagesHemodialysi S: Ariane Jake C. Fernandez, RN, MSNMicah Alexis Candelario100% (3)
- Drugs Affecting Renal SystemDocument44 pagesDrugs Affecting Renal SystemRwapembe StephenNo ratings yet
- Farmakoterapi Sistem RenalDocument89 pagesFarmakoterapi Sistem RenalNhovieNhowaaNo ratings yet
- HemodialysisDocument2 pagesHemodialysiselijahdale.guillergan-05No ratings yet
- A Review of Liver Anatomy and PhysiologyDocument41 pagesA Review of Liver Anatomy and PhysiologyVaseaPupchin0% (1)
- ICU Acute Kidney Injury & Mysthenia GravisDocument17 pagesICU Acute Kidney Injury & Mysthenia Gravisf6080683No ratings yet
- Toxocology: Abdullah Alolayan, R4Document6 pagesToxocology: Abdullah Alolayan, R4soulstakersNo ratings yet
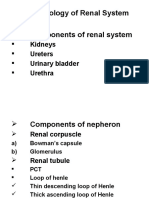
- Pharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraDocument30 pagesPharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraMirza HassanNo ratings yet
- Share Mszo113 - Animal-Wps OfficeDocument29 pagesShare Mszo113 - Animal-Wps OfficeRoopa Ram MundhanNo ratings yet
- DIURETICS LECTURE ZebDocument52 pagesDIURETICS LECTURE ZebPROF DR SHAHMURAD100% (2)
- Presentation On Diuretics+synthesis Final VersionDocument58 pagesPresentation On Diuretics+synthesis Final VersionArkw ChakrabortyNo ratings yet
- Diuretic Drugs: Thiazides Sites of ActionDocument52 pagesDiuretic Drugs: Thiazides Sites of Actionuzzal ahmedNo ratings yet
- PhisyologyDocument10 pagesPhisyologyAhmed MoghazyNo ratings yet
- 10 ExcretionDocument3 pages10 ExcretionKavin ManimaranNo ratings yet
- Kidney PathophysiologyDocument19 pagesKidney PathophysiologyGeorge MKNo ratings yet
- Dialysis PrescriptionDocument23 pagesDialysis PrescriptionMercy Juliana Jacqualine100% (1)
- Function of KidneyDocument66 pagesFunction of KidneyNilesh100% (4)
- OLIGURIADocument31 pagesOLIGURIAAnnushika PalanichamyNo ratings yet
- Dialysis Dose Prescription: Presented by Dr. UjjawalDocument54 pagesDialysis Dose Prescription: Presented by Dr. UjjawalZH. omg sarNo ratings yet
- Loop DiureticsDocument16 pagesLoop DiureticsMuhammad ZamimNo ratings yet
- What Is: Acute Kidney InjuryDocument31 pagesWhat Is: Acute Kidney InjuryDanielle KayeNo ratings yet
- Understanding Acute Kidney Injury and Renal FailureDocument32 pagesUnderstanding Acute Kidney Injury and Renal FailureCiedelle Honey Lou DimaligNo ratings yet
- Types and Procedures of DialysisDocument8 pagesTypes and Procedures of DialysisKristine PangahinNo ratings yet
- Lecture 4 Mechanism of Renal ExcretionDocument16 pagesLecture 4 Mechanism of Renal ExcretionNimra WNo ratings yet
- Sec1 Clinical2 (ARF)Document44 pagesSec1 Clinical2 (ARF)ahmedmohamed01153159469No ratings yet
- DiureticsDocument10 pagesDiureticsSantosh RoyNo ratings yet
- 2687pharmacy Lecture 2Document61 pages2687pharmacy Lecture 2Eman QawasmiNo ratings yet
- Lecture 9Document14 pagesLecture 9Aan KurniawanNo ratings yet
- Routes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary ExcretionDocument5 pagesRoutes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary Excretiontanuja reddyNo ratings yet
- Electrolyte and Fluid Balance: Understanding Intake, Output, Transport and ImbalancesDocument38 pagesElectrolyte and Fluid Balance: Understanding Intake, Output, Transport and ImbalancesMalika SadridinovaNo ratings yet
- Dialysis Notes 1Document3 pagesDialysis Notes 1SarahSigrid87% (23)
- Diuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowDocument35 pagesDiuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowAmanuel Maru100% (1)
- Renal Emergencies & Renal Replacement TherapyDocument58 pagesRenal Emergencies & Renal Replacement TherapyNilanka PiumalNo ratings yet
- Drug Elimination in KidneyDocument24 pagesDrug Elimination in KidneyRabail GalaniNo ratings yet
- 2021 Farmasi Sistem UrinariaDocument93 pages2021 Farmasi Sistem UrinariaRayhan NugrahaNo ratings yet
- Artificial Kidney: Hamid Naseem MD Sohrab Ansari Department of Electrical EngineeringDocument28 pagesArtificial Kidney: Hamid Naseem MD Sohrab Ansari Department of Electrical EngineeringHamid Naseem100% (1)
- DFD L5Document54 pagesDFD L5yousernameNo ratings yet
- Wear protective clothing to avoid secondary contaminationDocument46 pagesWear protective clothing to avoid secondary contaminationyousernameNo ratings yet
- Toxicology Lecture 5 - DigoxinDocument29 pagesToxicology Lecture 5 - DigoxinyousernameNo ratings yet
- Emergency Management of Toxicity: ABCDE, Decontamination, AntidotesDocument47 pagesEmergency Management of Toxicity: ABCDE, Decontamination, AntidotesyousernameNo ratings yet
- Sequence AlignmentDocument44 pagesSequence AlignmentyousernameNo ratings yet
- Pharmacy Management: by Hesham Shazly, PHD Semester Two BueDocument20 pagesPharmacy Management: by Hesham Shazly, PHD Semester Two BueyousernameNo ratings yet
- Botany Lecture 4Document23 pagesBotany Lecture 4yousernameNo ratings yet
- Phytotherapy RSDocument34 pagesPhytotherapy RSyousernameNo ratings yet
- Toxicology (Lecture 1)Document42 pagesToxicology (Lecture 1)yousernameNo ratings yet
- Phytotherapy NSDocument29 pagesPhytotherapy NSyousernameNo ratings yet
- Toxicology Lecture 7 Fe ToxicityDocument20 pagesToxicology Lecture 7 Fe ToxicityyousernameNo ratings yet
- Phytotherapy GIT (17-18.NEW)Document38 pagesPhytotherapy GIT (17-18.NEW)yousernameNo ratings yet
- Mo3jam Albalagha Al3arabiya 1Document503 pagesMo3jam Albalagha Al3arabiya 1yousernameNo ratings yet
- Serology 1Document28 pagesSerology 1yousernameNo ratings yet
- Biostatistics (L-7) : Mohey Elmazar Professor of Pharmacology & Toxicology Dean of Pharmacy (BUE)Document12 pagesBiostatistics (L-7) : Mohey Elmazar Professor of Pharmacology & Toxicology Dean of Pharmacy (BUE)yousernameNo ratings yet
- Cology 1Document6 pagesCology 1yousernameNo ratings yet
- (Cambridge Studies in Cognitive Linguistics) Jeannette Littlemore-Metonymy - Hidden Shortcuts in Language, Thought and Communication-Cambridge University PressDocument242 pages(Cambridge Studies in Cognitive Linguistics) Jeannette Littlemore-Metonymy - Hidden Shortcuts in Language, Thought and Communication-Cambridge University PressIvana100% (10)
- Pharmacy Management Lecture 10Document27 pagesPharmacy Management Lecture 10yousernameNo ratings yet
- Drug Design (ELECTIVE) - Lecture 2Document28 pagesDrug Design (ELECTIVE) - Lecture 2yousernameNo ratings yet
- Drug Design Lecture1Document23 pagesDrug Design Lecture1yousernameNo ratings yet
- Stat Lecture 1Document16 pagesStat Lecture 1yousernameNo ratings yet
- Molecular Biology Tuotorial - RNA Extraction RT-PCRDocument30 pagesMolecular Biology Tuotorial - RNA Extraction RT-PCRyousernameNo ratings yet
- Gene Therapy 3-4-2016Document43 pagesGene Therapy 3-4-2016yousernameNo ratings yet
- Anatomy MidtermDocument6 pagesAnatomy MidtermyousernameNo ratings yet
- Lecture 5,6Document12 pagesLecture 5,6yousernameNo ratings yet
- Molecular Biology Tutorial 11-10-2015.Ppt FinalDocument30 pagesMolecular Biology Tutorial 11-10-2015.Ppt FinalyousernameNo ratings yet
- Questions For Training IIDocument1 pageQuestions For Training IIyousernameNo ratings yet
- Analytical Chem. Methods for Qualitative AnalysisDocument13 pagesAnalytical Chem. Methods for Qualitative AnalysisyousernameNo ratings yet
- SAIDI Ball Valves Eng PDFDocument180 pagesSAIDI Ball Valves Eng PDFtrifiloNo ratings yet
- Chip FormationDocument27 pagesChip FormationJasvinder SinghNo ratings yet
- Analisis Risisko Kesehatan Pajanan Benzena Di Industri Percetakan X Kota SemarangDocument8 pagesAnalisis Risisko Kesehatan Pajanan Benzena Di Industri Percetakan X Kota SemarangAyunda SaputriNo ratings yet
- Uniflor Brochure English72Document6 pagesUniflor Brochure English72gaggy1983No ratings yet
- Jurnal Eucast LainnyaDocument228 pagesJurnal Eucast Lainnyaonly taaNo ratings yet
- National Eggshell Emulsion (Matt)Document4 pagesNational Eggshell Emulsion (Matt)PJ PJNo ratings yet
- Oxford Instruments - PMI-MASTER Pro2Document4 pagesOxford Instruments - PMI-MASTER Pro2NAdreaNo ratings yet
- Sunbrella Upholstery Fabric 2018-2020 ENDocument43 pagesSunbrella Upholstery Fabric 2018-2020 ENMark Anthony DingalNo ratings yet
- A Guide To Glycols - DowDocument58 pagesA Guide To Glycols - DowvoromarNo ratings yet
- Magnasoft JSSDocument5 pagesMagnasoft JSSLe LocNo ratings yet
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- Types of Titration CurvesDocument63 pagesTypes of Titration CurvesVibhinn SinghalNo ratings yet
- Effects of mineral additives on concrete properties determined via Taguchi methodDocument9 pagesEffects of mineral additives on concrete properties determined via Taguchi methodAhmet SevinçNo ratings yet
- RTV Solutions BrochureDocument27 pagesRTV Solutions BrochureJaques JaquesNo ratings yet
- An Overview of The Modified Chemical Vapor Deposition (MCVD) Process and Performance - 2Document18 pagesAn Overview of The Modified Chemical Vapor Deposition (MCVD) Process and Performance - 2Nguyen TheanhNo ratings yet
- Designing of A TPH Fire Tube Boiler: December 2019Document25 pagesDesigning of A TPH Fire Tube Boiler: December 2019Hélder PascoalNo ratings yet
- Food Hydrocolloids: Alejandra Agudelo, Paula Varela, Teresa Sanz, Susana FiszmanDocument11 pagesFood Hydrocolloids: Alejandra Agudelo, Paula Varela, Teresa Sanz, Susana Fiszmanmax693No ratings yet
- Fenoterol HydrobromideDocument2 pagesFenoterol HydrobromideAnonymous XgX8kTNo ratings yet
- For Storage & Management of LubricantsDocument7 pagesFor Storage & Management of LubricantsPrajyot MahajanNo ratings yet
- EutrophicationDocument8 pagesEutrophicationashuchemNo ratings yet
- Bellows Suction Cup NBR (Round) : SAB 30 NBR-60 G1/4-IGDocument2 pagesBellows Suction Cup NBR (Round) : SAB 30 NBR-60 G1/4-IGAndor TorokNo ratings yet
- Mixtures Pure and Impure Substances Homework Activity Sheet - Ver - 2Document2 pagesMixtures Pure and Impure Substances Homework Activity Sheet - Ver - 2Sarah KKCNo ratings yet
- Afrc 1993Document91 pagesAfrc 1993Claudio Luiz de Souza89% (9)
- Lab Report: Shahjalal University of Science & Technology, SylhetDocument6 pagesLab Report: Shahjalal University of Science & Technology, SylhetMd Afif AbrarNo ratings yet
- Urea Reactor Designing: Chemical EngineeringDocument15 pagesUrea Reactor Designing: Chemical Engineeringalok sahuNo ratings yet
- J 05Document20 pagesJ 05Rochdi SahliNo ratings yet
- Asme Sec Viii D1 C PT UhtDocument14 pagesAsme Sec Viii D1 C PT Uhtkcp1986No ratings yet
- There Are No Incurable DiseasesDocument112 pagesThere Are No Incurable DiseasesAleksandra Milosevic100% (47)
- Bourdon Tube Pressure Gauge Stainless Steel Case Type 212.53 - Dry Case Type 213.53 - Liquid-Filled CaseDocument3 pagesBourdon Tube Pressure Gauge Stainless Steel Case Type 212.53 - Dry Case Type 213.53 - Liquid-Filled CasecarlosNo ratings yet
- LEUNG, Shuk-Ching, Jessica - Analysis of Changes in Starch ++ Post-Fermentation of Opaque Sorhgum Beer - 2002Document114 pagesLEUNG, Shuk-Ching, Jessica - Analysis of Changes in Starch ++ Post-Fermentation of Opaque Sorhgum Beer - 2002ninkasi1No ratings yet