You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Noise Induced Hearing LossDocument13 pagesNoise Induced Hearing LossanggashredNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ovarian CystDocument26 pagesOvarian CystAlmyr RimandoNo ratings yet
- Cristina Barsolo VS SSSDocument2 pagesCristina Barsolo VS SSSHasmer Maulana AmalNo ratings yet
- Lymph Drainage For DetoxificationDocument8 pagesLymph Drainage For DetoxificationJay JonesNo ratings yet
- Decision Making For Tooth Extraction or ConservationDocument16 pagesDecision Making For Tooth Extraction or Conservationavi_sdc100% (1)
- Maternal & Child Health Nursing Exam 7: NLE Pre-Boards (100 Items)Document35 pagesMaternal & Child Health Nursing Exam 7: NLE Pre-Boards (100 Items)cha mcbNo ratings yet
- VBAC MCQsDocument3 pagesVBAC MCQsHanaNo ratings yet
- CRISPR/Cas9 Genome Editing Tool: Potential Applications in Ophthalmologic Genome SurgeryDocument14 pagesCRISPR/Cas9 Genome Editing Tool: Potential Applications in Ophthalmologic Genome SurgeryAioanei CasianNo ratings yet
- Drug Study CEFAZOLINDocument6 pagesDrug Study CEFAZOLINAicelle Love Sampat LapenaNo ratings yet
- DAFTAR PUSTAKA - PUTRI UTAMI - BIOLOGI'17-dikonversiDocument3 pagesDAFTAR PUSTAKA - PUTRI UTAMI - BIOLOGI'17-dikonversiThoriqNo ratings yet
- Practice Test 2 1st Sem 2013Document11 pagesPractice Test 2 1st Sem 2013Isabel Barredo Del MundoNo ratings yet
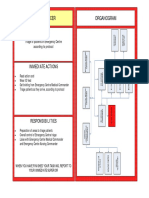
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Chapter 14: Principles of Disease and EpidemiologyDocument53 pagesChapter 14: Principles of Disease and EpidemiologyAbhishek Isaac MathewNo ratings yet
- Nutrient-Drug Interactions and FoodDocument5 pagesNutrient-Drug Interactions and FoodRijantono Franciscus MariaNo ratings yet
- Anc Guideline Feb 24 2022Document80 pagesAnc Guideline Feb 24 2022ASHENAFI LEMESANo ratings yet
- Systematic ReviewDocument11 pagesSystematic ReviewYuni PurwatiningsihNo ratings yet
- Difference Between Pulpotomy and PulpectomyDocument4 pagesDifference Between Pulpotomy and PulpectomyAnonymous Sb7suHTWNo ratings yet
- Oh ManDocument2 pagesOh ManDaniel LaurenteNo ratings yet
- Sarkar KC and Biswas MCDocument7 pagesSarkar KC and Biswas MCDr. Shashwat BhattacharyyaNo ratings yet
- Dose ResponseDocument42 pagesDose ResponseHend maarofNo ratings yet
- Trendelenburg PositionDocument2 pagesTrendelenburg PositionCudith LofinciNo ratings yet
- Why Can't A Man Become Pregnant?Document2 pagesWhy Can't A Man Become Pregnant?BSN 2 - Sasis, Rusmaryte C.No ratings yet
- Powerpoint: Colorectal Surgical DiseasesDocument74 pagesPowerpoint: Colorectal Surgical Diseasesj.doe.hex_87100% (1)
- RCDSO Standard of Practice Dental CT ScannersDocument8 pagesRCDSO Standard of Practice Dental CT Scannersl4j0b9No ratings yet
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocument41 pagesAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junNo ratings yet
- Prolonged Labour - Print DR AdilDocument2 pagesProlonged Labour - Print DR AdilAri Puji AstutiNo ratings yet
- Clinical Application of A Stereolithographic Surgical Guide For Simple Positioning of Orthodontic Mini-Implants.Document12 pagesClinical Application of A Stereolithographic Surgical Guide For Simple Positioning of Orthodontic Mini-Implants.Minh ĐạtNo ratings yet
- Benign Prostatic Hyperplasia (BPH) : Hyperplasia: Diagnosis and Treatment (1994) Was The Starting Point ForDocument14 pagesBenign Prostatic Hyperplasia (BPH) : Hyperplasia: Diagnosis and Treatment (1994) Was The Starting Point ForAnemiaHemolyticNo ratings yet
- Glasgow Coma Scale Canvas NCM 116 SkillsDocument6 pagesGlasgow Coma Scale Canvas NCM 116 Skillsbing bongNo ratings yet
- Radiologic Pathology Intro 1Document50 pagesRadiologic Pathology Intro 1James MoralesNo ratings yet