You might also like
- Cline y Angier (2010) - The Arvon Book of Life Writing. Writing Biography, Autobiography and MemoirDocument289 pagesCline y Angier (2010) - The Arvon Book of Life Writing. Writing Biography, Autobiography and MemoirConstanza Arraño100% (5)
- Customer Experience For DummiesDocument51 pagesCustomer Experience For DummiesAlejandroNo ratings yet
- 11-C3 Aging FaceDocument68 pages11-C3 Aging Facesalibagustavo100% (1)
- Ralph Alan Dale 1972 Hypnotism and EducationDocument21 pagesRalph Alan Dale 1972 Hypnotism and EducationFrancis Gladstone-Quintuplet100% (2)
- UntitledDocument385 pagesUntitledDelta BravoNo ratings yet
- Ccie DC Full Scale Labs PDFDocument185 pagesCcie DC Full Scale Labs PDFnaveedrana100% (2)
- 1908 The Watchower and Herald of Christ's PresenceDocument193 pages1908 The Watchower and Herald of Christ's PresenceTimothy RichesNo ratings yet
- Aging Skin Fore 06Document12 pagesAging Skin Fore 06Felp ScholzNo ratings yet
- Case Presentation: Placenta Previa: Crissa Marie D. PinedaDocument42 pagesCase Presentation: Placenta Previa: Crissa Marie D. PinedaCrissa PinedaNo ratings yet
- Unit 5 and 6Document2 pagesUnit 5 and 6Leo GonellNo ratings yet
- Nursing Case Study - 1 - (Acs)Document32 pagesNursing Case Study - 1 - (Acs)nidhiNo ratings yet
- Week 2 Day 1 GRADE 8Document2 pagesWeek 2 Day 1 GRADE 8Anonymous yElhvOhPnNo ratings yet
- OVERVIEWDocument16 pagesOVERVIEWjae eNo ratings yet
- Collagen Supplementation For Skin Health: A Mechanistic Systematic Review - 2020Document10 pagesCollagen Supplementation For Skin Health: A Mechanistic Systematic Review - 2020ranasoftNo ratings yet
- Hard Water and Cleansers An Invitro Study of The Effects On Immature Reconstructed Human Epidermis 1044Document8 pagesHard Water and Cleansers An Invitro Study of The Effects On Immature Reconstructed Human Epidermis 1044Alisher YermekNo ratings yet
- Nutrients 12 00870 v2Document25 pagesNutrients 12 00870 v2Caroline OktarinaNo ratings yet
- Oral Collagen Supplements Intake On Improving Skin Structure and FunctionDocument7 pagesOral Collagen Supplements Intake On Improving Skin Structure and FunctionDEEVA SKINCARENo ratings yet
- Carboxi Regeneracion de ColagenoDocument6 pagesCarboxi Regeneracion de ColagenoContacto AllA-MedicalNo ratings yet
- Czajka 2018Document12 pagesCzajka 2018jordan ulloa belloNo ratings yet
- Biofactors - Paperq10 2016Document10 pagesBiofactors - Paperq10 2016DEEVA SKINCARENo ratings yet
- Infant Skin Barrier, Structure, and Enzymatic Activity Differ From Those of Adult in An East Asian CohortDocument8 pagesInfant Skin Barrier, Structure, and Enzymatic Activity Differ From Those of Adult in An East Asian CohortS FznsNo ratings yet
- Colladerm 1 PDFDocument5 pagesColladerm 1 PDFnilesh borkarNo ratings yet
- Oral Intake LMW Collagen PeptideDocument13 pagesOral Intake LMW Collagen PeptideDEEVA SKINCARENo ratings yet
- Enhancing Skin Health: by Oral Administration of Natural Compounds and Minerals With Implications To The Dermal MicrobiomeDocument35 pagesEnhancing Skin Health: by Oral Administration of Natural Compounds and Minerals With Implications To The Dermal MicrobiomeMiruna Deleanu MariaNo ratings yet
- Oral Collagen Supplementation For Skin Aging: A Fad or The Future?Document3 pagesOral Collagen Supplementation For Skin Aging: A Fad or The Future?monitamiftahNo ratings yet
- Cytokines and The Skin Barrier: Molecular SciencesDocument26 pagesCytokines and The Skin Barrier: Molecular SciencesFelp ScholzNo ratings yet
- The Infant Skin Barrier Can We Preserve, Protect, and Enhance The BarrierDocument18 pagesThe Infant Skin Barrier Can We Preserve, Protect, and Enhance The Barrieranon_57137216No ratings yet
- Correia 2021Document24 pagesCorreia 2021LatifaNo ratings yet
- Elastin Structure and Its Involvemnt in Skin PhotoageingDocument7 pagesElastin Structure and Its Involvemnt in Skin PhotoageingEka LimNo ratings yet
- Bio MetilDocument20 pagesBio Metilsimone toledoNo ratings yet
- 2020 Oral Collagen Drinks For AntiagingDocument9 pages2020 Oral Collagen Drinks For AntiaginganonNo ratings yet
- Geriatric Nursing: Feature ArticleDocument5 pagesGeriatric Nursing: Feature ArticleBryan NguyenNo ratings yet
- DLMDocument14 pagesDLMEmmanuel BrizuelaNo ratings yet
- AntioxidantesDocument7 pagesAntioxidantesSilvana OliveiraNo ratings yet
- In Uence of Aqueous Cream BP On Corneocyte Size, Maturity, Skin Protease Activity, Protein Content and Transepidermal Water LossDocument7 pagesIn Uence of Aqueous Cream BP On Corneocyte Size, Maturity, Skin Protease Activity, Protein Content and Transepidermal Water LossFenni OktoberryNo ratings yet
- Buy Natural Skin CareDocument5 pagesBuy Natural Skin CarehershelritchNo ratings yet
- Effect of Topical Clay Application On The Synthesis of Collagen in SkinDocument5 pagesEffect of Topical Clay Application On The Synthesis of Collagen in SkinFelp ScholzNo ratings yet
- Dr. Anjali EyeDocument64 pagesDr. Anjali EyeNaveen KumarNo ratings yet
- Effect of Chitosajournaln JournalDocument7 pagesEffect of Chitosajournaln JournalSabrina Ceasy AnggraeniNo ratings yet
- Collagen AntiwrinkleDocument6 pagesCollagen AntiwrinkleAgung PriyantoNo ratings yet
- Reverse Skin Aging Around Your Eyes: by Gary Goldfaden, MD, and Robert GoldfadenDocument6 pagesReverse Skin Aging Around Your Eyes: by Gary Goldfaden, MD, and Robert GoldfadenAlen AhsanNo ratings yet
- Skin Anti-Aging Strategies A ReviewDocument10 pagesSkin Anti-Aging Strategies A ReviewPUNA RAMNo ratings yet
- PROTEASYLDocument4 pagesPROTEASYLAlberto Espinosa HernándezNo ratings yet
- An Overview of The Beneficial Effects of HydrolyseDocument15 pagesAn Overview of The Beneficial Effects of Hydrolyse陳沂仿No ratings yet
- A Patobiologia Da Pele No Envelhecimento - American Pathology JournalDocument14 pagesA Patobiologia Da Pele No Envelhecimento - American Pathology JournalGermano Freire Bezerra FilhoNo ratings yet
- Skin HydrationDocument7 pagesSkin Hydrationade fitriyani lubisNo ratings yet
- Collagen Supplementation: Therapy For Skin Disorders: A ReviewDocument15 pagesCollagen Supplementation: Therapy For Skin Disorders: A ReviewJefferson OrtegaNo ratings yet
- 1 s2.0 S0923181121000840 MainDocument16 pages1 s2.0 S0923181121000840 Mainleon4009No ratings yet
- De Luca 2016 PDFDocument15 pagesDe Luca 2016 PDFiulianaNo ratings yet
- Antioxidants: Collagen Hydrolysates For Skin Protection: Oral Administration and Topical FormulationDocument17 pagesAntioxidants: Collagen Hydrolysates For Skin Protection: Oral Administration and Topical FormulationyadNo ratings yet
- J Clindermatol 2020 04 003Document7 pagesJ Clindermatol 2020 04 003R RahmadaniNo ratings yet
- ArticulosDocument10 pagesArticulosDⒶrk OtⒶkuNo ratings yet
- Efeitos Da Ingestão de Colágeno Hidrolisado Na PeleDocument5 pagesEfeitos Da Ingestão de Colágeno Hidrolisado Na PeleAdriana VasconcelosNo ratings yet
- Glutathione and It's Antiaging and Antimelanogenic Effects: BackgroundDocument14 pagesGlutathione and It's Antiaging and Antimelanogenic Effects: BackgroundFlor SarmientoNo ratings yet
- Seminar: The Roles of Vitamin C in Skin Health AbstractDocument7 pagesSeminar: The Roles of Vitamin C in Skin Health AbstractAnh TramNo ratings yet
- Characteristics of The Aging Skin: Critical ReviewsDocument6 pagesCharacteristics of The Aging Skin: Critical ReviewsRatih Anindita Rahajeng RipyonoNo ratings yet
- Importance of The Microenvironment and Mechanosensing in Adipose Tissue Biology 2022 ReviewDocument29 pagesImportance of The Microenvironment and Mechanosensing in Adipose Tissue Biology 2022 Review畏No ratings yet
- Fighting Against Skin Aging: The Way From Bench To Bedside: Shoubing Zhang and Enkui DuanDocument10 pagesFighting Against Skin Aging: The Way From Bench To Bedside: Shoubing Zhang and Enkui DuanRiley RilanNo ratings yet
- JCCD 2 128Document8 pagesJCCD 2 128Yohanes SuandriannoNo ratings yet
- A Review of Skin and The Effects of Aging On Skin Structure and Function - Skin Turnover TimeDocument10 pagesA Review of Skin and The Effects of Aging On Skin Structure and Function - Skin Turnover TimeEUNPYO LEENo ratings yet
- Lu Et Al., 2012Document7 pagesLu Et Al., 2012Tatiana DutraNo ratings yet
- Wound HealingDocument23 pagesWound HealingMarry M. MarquesNo ratings yet
- Mucoadhesive Drug Delivery System ThesisDocument8 pagesMucoadhesive Drug Delivery System Thesistracyjimenezstamford100% (2)
- Beneficial Long-Term Effects of CombinedDocument12 pagesBeneficial Long-Term Effects of CombinedAdriana VasconcelosNo ratings yet
- Artigo Açúcar X EnvelhecimentoDocument3 pagesArtigo Açúcar X EnvelhecimentoAline MoraesNo ratings yet
- Segregation of Age-Related Skin Microbiome Characteristics by FunctionalityDocument11 pagesSegregation of Age-Related Skin Microbiome Characteristics by Functionalitypka25No ratings yet
- Integration of Skin Phenome and Microbiome RevealsDocument23 pagesIntegration of Skin Phenome and Microbiome RevealsanaNo ratings yet
- Lawler 2019Document15 pagesLawler 2019Ulul AzmiNo ratings yet
- Out 3Document9 pagesOut 3Musthafa Afif WardhanaNo ratings yet
- A Cosmetic Approach To Cutaneous DefectsDocument22 pagesA Cosmetic Approach To Cutaneous DefectsStatiunea Balta AlbaNo ratings yet
- Patch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGFrom EverandPatch Testing and Prick Testing: A Practical Guide Official Publication of the ICDRGNo ratings yet
- Biofactors - Paperq10 2016Document10 pagesBiofactors - Paperq10 2016DEEVA SKINCARENo ratings yet
- Oral Intake LMW Collagen PeptideDocument13 pagesOral Intake LMW Collagen PeptideDEEVA SKINCARENo ratings yet
- Vitamin A and Carotenoid Toxicity: Rune BlomhoffDocument15 pagesVitamin A and Carotenoid Toxicity: Rune BlomhoffDEEVA SKINCARENo ratings yet
- Non Invasive Arm Fat ReductionDocument10 pagesNon Invasive Arm Fat ReductionDEEVA SKINCARENo ratings yet
- The Diagnostic Dilemma of Erythema Nodosum Leprosum - A Clinicohistological StudyDocument10 pagesThe Diagnostic Dilemma of Erythema Nodosum Leprosum - A Clinicohistological StudyDEEVA SKINCARENo ratings yet
- English Slide Un SMK 1819Document93 pagesEnglish Slide Un SMK 1819EkhaSoemarnoNo ratings yet
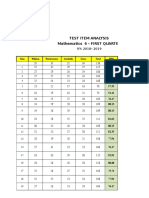
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet
- Ol7 SecurityDocument84 pagesOl7 Securityneaman_ahmedNo ratings yet
- Neonatal Phototherapy: Operator ManualDocument16 pagesNeonatal Phototherapy: Operator ManualAbel FencerNo ratings yet
- Usability Test Report MemoDocument2 pagesUsability Test Report MemoTiffany PetersonNo ratings yet
- Fender Re-Issue 62 Jazzmaster Wiring DiagramDocument1 pageFender Re-Issue 62 Jazzmaster Wiring DiagrambenitoNo ratings yet
- Biodiversity ReportDocument52 pagesBiodiversity ReportAdrian HudsonNo ratings yet
- Control Grupos Electrogenos LobatoDocument20 pagesControl Grupos Electrogenos LobatoEdwin Santiago Villegas AuquesNo ratings yet
- CHED - NYC PresentationDocument19 pagesCHED - NYC PresentationMayjee De La CruzNo ratings yet
- Caps 5Document4 pagesCaps 5shheNo ratings yet
- Pyneng Readthedocs Io en LatestDocument702 pagesPyneng Readthedocs Io en LatestNgọc Duy VõNo ratings yet
- Conscious Sedation PaediatricsDocument44 pagesConscious Sedation PaediatricsReeta TaxakNo ratings yet
- Children With Cochlear Implants The Communication JourneeyDocument22 pagesChildren With Cochlear Implants The Communication Journeeyismail39No ratings yet
- Line-And-Staff Organizations - Examples, Advantages, Manager, Type, Company, Disadvantages, BusinessDocument4 pagesLine-And-Staff Organizations - Examples, Advantages, Manager, Type, Company, Disadvantages, BusinessSangram PradhanNo ratings yet
- The Top Level Diagram Is A Use Case Diagram That Shows The Actors andDocument5 pagesThe Top Level Diagram Is A Use Case Diagram That Shows The Actors andsin2pNo ratings yet
- TDS - 0121 - CapaCare Classic - 201912Document5 pagesTDS - 0121 - CapaCare Classic - 201912ayviwurbayviwurbNo ratings yet
- Geologic Report Arches NationalDocument9 pagesGeologic Report Arches NationalJacob AndersonNo ratings yet
- (E) Chapter 1 - Origin of Soil and Grain SizeDocument23 pages(E) Chapter 1 - Origin of Soil and Grain SizeLynas Beh TahanNo ratings yet
- Citing SourcesDocument37 pagesCiting Sourcesasquared29No ratings yet