You might also like
- LED-Based Photoacoustic Imaging: From Bench to BedsideFrom EverandLED-Based Photoacoustic Imaging: From Bench to BedsideMithun Kuniyil Ajith SinghNo ratings yet
- Generating Report of Bone Fracture and Bleeding Using X-Ray ImagesDocument7 pagesGenerating Report of Bone Fracture and Bleeding Using X-Ray ImagesIJRASETPublicationsNo ratings yet
- Quantitative MRI of the Spinal CordFrom EverandQuantitative MRI of the Spinal CordJulien Cohen-AdadNo ratings yet
- Barber 2018Document4 pagesBarber 2018Boris CanahuireNo ratings yet
- Knee Osteoarthritis Detection and Severity Prediction Using Convolutional Neural NetworkDocument7 pagesKnee Osteoarthritis Detection and Severity Prediction Using Convolutional Neural NetworkIJRASETPublicationsNo ratings yet
- Applications of Machine Learning To Imaging of Spinal Disorders: Current Status and Future DirectionsDocument7 pagesApplications of Machine Learning To Imaging of Spinal Disorders: Current Status and Future DirectionsOTSMANE ChaimaaNo ratings yet
- Bone Erosion Scoring For Rheumatoid ArthritisDocument10 pagesBone Erosion Scoring For Rheumatoid Arthritisdas.sandipan5102002No ratings yet
- Eng-Cyst Detection in MRI Brain Image-Vrushali D. DharmaleDocument10 pagesEng-Cyst Detection in MRI Brain Image-Vrushali D. DharmaleImpact JournalsNo ratings yet
- Accountabilities of Digital Image Processing in Biomedical ImagingDocument6 pagesAccountabilities of Digital Image Processing in Biomedical ImagingIJRASETPublicationsNo ratings yet
- A - Hybrid - CNN-PH 2based - Segmentation - and - Boosting - Classifier - For - Real - Time - Sensor - Spinal - Cord - Injury - DataDocument10 pagesA - Hybrid - CNN-PH 2based - Segmentation - and - Boosting - Classifier - For - Real - Time - Sensor - Spinal - Cord - Injury - DataKarpagam KNo ratings yet
- Omicron Detection With X-Ray and CT-Scan Using Machine LearningDocument6 pagesOmicron Detection With X-Ray and CT-Scan Using Machine LearningIJRASETPublicationsNo ratings yet
- Spine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesDocument6 pagesSpine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesSandeep VermaNo ratings yet
- Iort 89 1453714Document7 pagesIort 89 1453714KARANAM SANTOSHNo ratings yet
- Artificial Intelligence in Ododontics Current Application and Future DirectionsDocument6 pagesArtificial Intelligence in Ododontics Current Application and Future DirectionsYoussef BoukhalNo ratings yet
- 2 Step Deep Learning Model For Landmarks Localization in Spine RadiographsDocument12 pages2 Step Deep Learning Model For Landmarks Localization in Spine Radiographsqiaowen wangNo ratings yet
- An Overview of Artificial Intelligence in Medical Physics and Radiation OncologyDocument11 pagesAn Overview of Artificial Intelligence in Medical Physics and Radiation Oncologyxiwevi4103No ratings yet
- S0016510721013213Document2 pagesS0016510721013213cifha rajesh saldanhaNo ratings yet
- Image Processing For Alzheimer's Disease DetectionDocument7 pagesImage Processing For Alzheimer's Disease DetectionIJRASETPublicationsNo ratings yet
- Automatic Detection of Knee Joints and Quantification of Knee Osteoarthritis Severity Using Modified Fully Connected Convolutional Neural NetworksDocument9 pagesAutomatic Detection of Knee Joints and Quantification of Knee Osteoarthritis Severity Using Modified Fully Connected Convolutional Neural NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Automatic Brain Tumor Detection Using Adaptive Region Growing With Thresholding MethodsDocument8 pagesAutomatic Brain Tumor Detection Using Adaptive Region Growing With Thresholding MethodsIAES IJAINo ratings yet
- Fuzzy Clustering Approach For Brain Tumor DetectionDocument8 pagesFuzzy Clustering Approach For Brain Tumor DetectionIJRASETPublicationsNo ratings yet
- JMC19013 36137Document15 pagesJMC19013 36137Waseem AbbasNo ratings yet
- A Systematic Review On Artificial Intelligence ForDocument20 pagesA Systematic Review On Artificial Intelligence ForblueyoonvNo ratings yet
- Retina Full DocumentDocument34 pagesRetina Full DocumentThe MindNo ratings yet
- Brain Tumour Detection Using The Deep LearningDocument8 pagesBrain Tumour Detection Using The Deep LearningIJRASETPublicationsNo ratings yet
- 1 - Alzheimer's Detection Through Neuro Imaging and Subsequent Fusion For Clinical DiagnosisDocument8 pages1 - Alzheimer's Detection Through Neuro Imaging and Subsequent Fusion For Clinical DiagnosisNguyễn Nhật-NguyênNo ratings yet
- Research Article: Detailed Shoulder MRI Findings in Manual Wheelchair Users With Shoulder PainDocument8 pagesResearch Article: Detailed Shoulder MRI Findings in Manual Wheelchair Users With Shoulder PainairusmayantiNo ratings yet
- Computerized Medical Imaging and GraphicsDocument8 pagesComputerized Medical Imaging and GraphicsMr.Mohammed Zakir B ELECTRONICS & COMMUNICATIONNo ratings yet
- Detection of Osteoarthritis Using Knee X-Ray ImageDocument8 pagesDetection of Osteoarthritis Using Knee X-Ray ImageAkbar aliNo ratings yet
- Machine Learning and Deep Learning in Medical Imaging: Intelligent ImagingDocument11 pagesMachine Learning and Deep Learning in Medical Imaging: Intelligent ImagingBreen Ramirez StrokesNo ratings yet
- Artificial Intelligence (AI) : What Are The Types of AI and How Do They Difer?Document2 pagesArtificial Intelligence (AI) : What Are The Types of AI and How Do They Difer?Shahrooz AmNo ratings yet
- Pi Is 2452109422001488Document10 pagesPi Is 2452109422001488Raul Matute MartinNo ratings yet
- MTPW DSM-410Document3 pagesMTPW DSM-410goutam1235No ratings yet
- Using Convolutional Neural Network To Design and Predict The Forces and Kinematic Performance and External Rotation Moment of The Hip Joint in The PelvisDocument6 pagesUsing Convolutional Neural Network To Design and Predict The Forces and Kinematic Performance and External Rotation Moment of The Hip Joint in The PelvisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 11.deep Learning Applications in Medical Image Analysis-Brain TumorDocument4 pages11.deep Learning Applications in Medical Image Analysis-Brain TumorVenky Naidu BalineniNo ratings yet
- Prediction of Alzheimer's Disease Using CNNDocument11 pagesPrediction of Alzheimer's Disease Using CNNIJRASETPublications100% (2)
- Radiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisDocument15 pagesRadiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisRaj PanchalNo ratings yet
- Accuracy of EOS Imagining Technology in Comparison.94031Document18 pagesAccuracy of EOS Imagining Technology in Comparison.94031Mohammad KaramNo ratings yet
- Journal Pone 0269931Document13 pagesJournal Pone 0269931Abdelali MoufidiNo ratings yet
- Artificial Intelligence (AI) in Urology-Current Use and Future Directions: An iTRUE StudyDocument13 pagesArtificial Intelligence (AI) in Urology-Current Use and Future Directions: An iTRUE StudyFicky HuangNo ratings yet
- Assign 03Document14 pagesAssign 03Aleeza AnjumNo ratings yet
- Httpssci Hub - Sedownloads2020!10!24e9athlani2020.pdfdownload TrueDocument9 pagesHttpssci Hub - Sedownloads2020!10!24e9athlani2020.pdfdownload TrueJosé Miguel Molina MárquezNo ratings yet
- Predicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDocument9 pagesPredicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDr-Rabia AlmamalookNo ratings yet
- Classification of Knee MRIDocument3 pagesClassification of Knee MRIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Goyal 2021 IOP Conf. Ser. Mater. Sci. Eng. 1022 012011Document10 pagesGoyal 2021 IOP Conf. Ser. Mater. Sci. Eng. 1022 012011Abhishek R BhatNo ratings yet
- Implementation of CT Image Segmentation Based On ADocument11 pagesImplementation of CT Image Segmentation Based On AZAHRA FASKANo ratings yet
- Orthod Craniofacial Res - 2021 - Bulatova - Assessment of Automatic Cephalometric Landmark Identification Using ArtificialDocument6 pagesOrthod Craniofacial Res - 2021 - Bulatova - Assessment of Automatic Cephalometric Landmark Identification Using ArtificialPaulusMetehNo ratings yet
- Digital Image Processing 222Document15 pagesDigital Image Processing 222Elizabeth JonesNo ratings yet
- Tumor DetectionDocument97 pagesTumor DetectionParthi Ban100% (1)
- A Brain Tumor Detection Using Image ProcessingDocument5 pagesA Brain Tumor Detection Using Image ProcessingIJRASETPublicationsNo ratings yet
- Pancreas Disease Detection and Segmentation Using Abdominal CT ScanDocument9 pagesPancreas Disease Detection and Segmentation Using Abdominal CT ScanIJAR JOURNALNo ratings yet
- Brain Tumour Classification and Identification Using Deep Learning Neural NetworksDocument6 pagesBrain Tumour Classification and Identification Using Deep Learning Neural NetworksIJRASETPublicationsNo ratings yet
- Applsci 11 06175Document22 pagesApplsci 11 06175Gurumoorthy KrishnamoorthyNo ratings yet
- Brain Mapping Disease Identification SystemDocument6 pagesBrain Mapping Disease Identification SystemIJRASETPublicationsNo ratings yet
- Efficient Lung Infection Detection Using Machine Learning ApproachDocument9 pagesEfficient Lung Infection Detection Using Machine Learning ApproachIJRASETPublicationsNo ratings yet
- 10 1097@iio 0000000000000298Document15 pages10 1097@iio 0000000000000298Mitcheel Lanas SozaNo ratings yet
- User-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityDocument49 pagesUser-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityNicholas KimNo ratings yet
- A Fuzzy C Means Clustering Approach For Gesture Recognition in HealthcareDocument8 pagesA Fuzzy C Means Clustering Approach For Gesture Recognition in HealthcarekrishnanandNo ratings yet
- Artificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglDocument2 pagesArtificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglMomoh GaiusNo ratings yet
- A UWB Antenna For Microwave Brain ImagingDocument2 pagesA UWB Antenna For Microwave Brain ImagingPr eeTNo ratings yet
- Internal Fixation of The Lumbar Spine With Pedicle.3Document11 pagesInternal Fixation of The Lumbar Spine With Pedicle.3lauraserranogonzalez517No ratings yet
- Lumbar SpineDocument43 pagesLumbar SpineVidhushi Vedhara100% (1)
- 6.S, R, U Systems of Female PelvisDocument2 pages6.S, R, U Systems of Female Pelvisahmned A DOCTORNo ratings yet
- Skeletal System: I. General CharacteristicsDocument34 pagesSkeletal System: I. General CharacteristicsMason BruceNo ratings yet
- Pp. vs. BanhaonDocument20 pagesPp. vs. BanhaonDelia PeabodyNo ratings yet
- Sci ReportDocument43 pagesSci ReportFaith BugtongNo ratings yet
- MVP Chapter 20 External Causes Morbidity April 2014 PDFDocument55 pagesMVP Chapter 20 External Causes Morbidity April 2014 PDFAnchal NigamNo ratings yet
- ANAT20006 2020: MSK Practice Quiz Short Answer Question Model AnswersDocument3 pagesANAT20006 2020: MSK Practice Quiz Short Answer Question Model AnswersJenniferChenNo ratings yet
- Henry Vernon Crock M.D., M.S., F.R.C.S., F.R.a.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983)Document334 pagesHenry Vernon Crock M.D., M.S., F.R.C.S., F.R.a.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983)Ionut VladNo ratings yet
- Spinal Cord Gross Anatomy 2Document40 pagesSpinal Cord Gross Anatomy 2Mohamad NasrullohNo ratings yet
- Mark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Document626 pagesMark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Suhani Mihai100% (1)
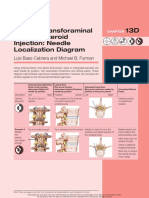
- Lumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramDocument2 pagesLumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramSoumabho DasNo ratings yet
- Morariu DDDprelimASN (1) (Compatibility Mode)Document25 pagesMorariu DDDprelimASN (1) (Compatibility Mode)SAKSHI KATIYARNo ratings yet
- Spinal Cystic SchwannomaDocument3 pagesSpinal Cystic SchwannomahelenNo ratings yet
- Textbook Reading (THE SPINE BY ROTHMANDocument73 pagesTextbook Reading (THE SPINE BY ROTHMANLanny F. TjioeNo ratings yet
- Anatomy MCQS Part 3 PDFDocument10 pagesAnatomy MCQS Part 3 PDFSamer Qusay100% (1)
- Facet Joint SyndromeDocument17 pagesFacet Joint Syndromepaulvaso27100% (1)
- Chir12006 Week 7 Study Guide Answers 1 3Document8 pagesChir12006 Week 7 Study Guide Answers 1 3api-469904011No ratings yet
- Anatomy AssignDocument25 pagesAnatomy AssignAdarshBijapurNo ratings yet
- Dunway Test PaperDocument73 pagesDunway Test PaperShivendu Sharma92% (12)
- Vertebral ColumnDocument84 pagesVertebral ColumnGenesis GeronagaNo ratings yet
- 10 Lumbosacral SpineDocument10 pages10 Lumbosacral Spine楊畯凱No ratings yet
- A Biomechanical Comparison of Lifting Techniques Between Subjects With and Without Chronic Low Back Pain During Freestyle Lifting and Lowering TasksDocument10 pagesA Biomechanical Comparison of Lifting Techniques Between Subjects With and Without Chronic Low Back Pain During Freestyle Lifting and Lowering TasksergoshaunNo ratings yet
- Regional Anesthesia in Cattle PDFDocument33 pagesRegional Anesthesia in Cattle PDFNiaz AsgharNo ratings yet
- Bertolotti's Syndrome - Diagnosis and ManagementDocument4 pagesBertolotti's Syndrome - Diagnosis and ManagementIOSRjournalNo ratings yet
- Free Hand Technique Lumbar Spine Pedicle Screw Placement in Indian PopulationDocument5 pagesFree Hand Technique Lumbar Spine Pedicle Screw Placement in Indian PopulationMaharajothiNo ratings yet
- Thomas Jonnesco - Remarks On General Spinal Analgesia (1909) .Document6 pagesThomas Jonnesco - Remarks On General Spinal Analgesia (1909) .BigBoss_GRUNo ratings yet
- BiomechanicsDocument59 pagesBiomechanicsMuqeet76No ratings yet
- Appleton & Lange Review of Anatomy PDFDocument157 pagesAppleton & Lange Review of Anatomy PDFherry2sw100% (2)
- Extra PointsDocument7 pagesExtra Pointspeter911x100% (2)
- The Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldFrom EverandThe Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldRating: 4.5 out of 5 stars4.5/5 (107)
- Artificial Intelligence: A Guide for Thinking HumansFrom EverandArtificial Intelligence: A Guide for Thinking HumansRating: 4.5 out of 5 stars4.5/5 (30)
- Working with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)From EverandWorking with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)Rating: 5 out of 5 stars5/5 (5)
- The AI Advantage: How to Put the Artificial Intelligence Revolution to WorkFrom EverandThe AI Advantage: How to Put the Artificial Intelligence Revolution to WorkRating: 4 out of 5 stars4/5 (7)
- Scary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldFrom EverandScary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldRating: 4.5 out of 5 stars4.5/5 (55)
- Generative AI: The Insights You Need from Harvard Business ReviewFrom EverandGenerative AI: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (3)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- HBR's 10 Must Reads on AI, Analytics, and the New Machine AgeFrom EverandHBR's 10 Must Reads on AI, Analytics, and the New Machine AgeRating: 4.5 out of 5 stars4.5/5 (69)
- Artificial Intelligence: The Insights You Need from Harvard Business ReviewFrom EverandArtificial Intelligence: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (104)
- T-Minus AI: Humanity's Countdown to Artificial Intelligence and the New Pursuit of Global PowerFrom EverandT-Minus AI: Humanity's Countdown to Artificial Intelligence and the New Pursuit of Global PowerRating: 4 out of 5 stars4/5 (4)
- Four Battlegrounds: Power in the Age of Artificial IntelligenceFrom EverandFour Battlegrounds: Power in the Age of Artificial IntelligenceRating: 5 out of 5 stars5/5 (5)
- Artificial Intelligence & Generative AI for Beginners: The Complete GuideFrom EverandArtificial Intelligence & Generative AI for Beginners: The Complete GuideRating: 5 out of 5 stars5/5 (1)
- 100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziFrom Everand100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziNo ratings yet
- Our Final Invention: Artificial Intelligence and the End of the Human EraFrom EverandOur Final Invention: Artificial Intelligence and the End of the Human EraRating: 4 out of 5 stars4/5 (82)
- System Design Interview: 300 Questions And Answers: Prepare And PassFrom EverandSystem Design Interview: 300 Questions And Answers: Prepare And PassNo ratings yet
- Competing in the Age of AI: Strategy and Leadership When Algorithms and Networks Run the WorldFrom EverandCompeting in the Age of AI: Strategy and Leadership When Algorithms and Networks Run the WorldRating: 4.5 out of 5 stars4.5/5 (21)
- How to Make Money Online Using ChatGPT Prompts: Secrets Revealed for Unlocking Hidden Opportunities. Earn Full-Time Income Using ChatGPT with the Untold Potential of Conversational AI.From EverandHow to Make Money Online Using ChatGPT Prompts: Secrets Revealed for Unlocking Hidden Opportunities. Earn Full-Time Income Using ChatGPT with the Untold Potential of Conversational AI.No ratings yet
- MidJourney Magnified: Crafting Visual Magic – The Novice to Pro PlaybookFrom EverandMidJourney Magnified: Crafting Visual Magic – The Novice to Pro PlaybookNo ratings yet
- Rise of Generative AI and ChatGPT: Understand how Generative AI and ChatGPT are transforming and reshaping the business world (English Edition)From EverandRise of Generative AI and ChatGPT: Understand how Generative AI and ChatGPT are transforming and reshaping the business world (English Edition)No ratings yet
- Hands-On System Design: Learn System Design, Scaling Applications, Software Development Design Patterns with Real Use-CasesFrom EverandHands-On System Design: Learn System Design, Scaling Applications, Software Development Design Patterns with Real Use-CasesNo ratings yet
- ChatGPT 4 $10,000 per Month #1 Beginners Guide to Make Money Online Generated by Artificial IntelligenceFrom EverandChatGPT 4 $10,000 per Month #1 Beginners Guide to Make Money Online Generated by Artificial IntelligenceNo ratings yet
- How To: GPT-4 for Financial Freedom: The Entrepreneur's Guide to Thriving in the AI EraFrom EverandHow To: GPT-4 for Financial Freedom: The Entrepreneur's Guide to Thriving in the AI EraRating: 4 out of 5 stars4/5 (9)
- AI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceFrom EverandAI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceRating: 4 out of 5 stars4/5 (2)