You might also like
- Nonabdominal Causes of Abdominal Pain: Finding Your Heart in Your Stomach!Document4 pagesNonabdominal Causes of Abdominal Pain: Finding Your Heart in Your Stomach!octa dikhoNo ratings yet
- 2007 Sizer, Cook, Brismeé - Screening For Red Flags in The Diagnosis and Management of MSK Spine PainDocument19 pages2007 Sizer, Cook, Brismeé - Screening For Red Flags in The Diagnosis and Management of MSK Spine PainRodrigo Suarez MartinezNo ratings yet
- Winzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Document5 pagesWinzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Tom StevensNo ratings yet
- Jama 268 6 030Document6 pagesJama 268 6 030Thiago Scharth MontenegroNo ratings yet
- Chronic Fatigue Syndrome From Chronic Fatigue To More Specific SyndromesDocument5 pagesChronic Fatigue Syndrome From Chronic Fatigue To More Specific SyndromesArgenis SalinasNo ratings yet
- A Practical Guide To Geriatric Syndromes in Older Adults With Cancer: A Focus On Falls, Cognition, Polypharmacy, and DepressionDocument14 pagesA Practical Guide To Geriatric Syndromes in Older Adults With Cancer: A Focus On Falls, Cognition, Polypharmacy, and DepressionShirleyNo ratings yet
- Symposium Article: Psychological Aspects of Depression in Cancer Patients: An UpdateDocument4 pagesSymposium Article: Psychological Aspects of Depression in Cancer Patients: An UpdateMel Izhra N. MargateNo ratings yet
- An Approach To The Patient With Chronic Undiagnosed Abdominal PainDocument7 pagesAn Approach To The Patient With Chronic Undiagnosed Abdominal PainCarlos Arturo Caparo ChallcoNo ratings yet
- Cardiovascular Disease: Chest Pain: Cardiac or NotDocument7 pagesCardiovascular Disease: Chest Pain: Cardiac or Notmahaberani_zNo ratings yet
- 2021 BJMO Geriatric Syndromes in OncologyDocument8 pages2021 BJMO Geriatric Syndromes in OncologyTarafainy BasalamahNo ratings yet
- Marin 2020Document38 pagesMarin 2020Tarek Ibrahim AlshihabiNo ratings yet
- Cleveland Clinic Journal of Medicine 2007 Klineberg 905 13Document9 pagesCleveland Clinic Journal of Medicine 2007 Klineberg 905 13Sohaib AliNo ratings yet
- Deyo 1992Document6 pagesDeyo 1992Wwwanand111No ratings yet
- American College of Gastroenterology Guidelines: Management of Acute PancreatitisDocument16 pagesAmerican College of Gastroenterology Guidelines: Management of Acute PancreatitisCarinka VidañosNo ratings yet
- Brief Resolved Unexplained Event: Child Health UpdateDocument3 pagesBrief Resolved Unexplained Event: Child Health UpdateNATALIA LEMOS CALLENo ratings yet
- S GSDTBNDFNZFDDocument14 pagesS GSDTBNDFNZFDnon_zenseNo ratings yet
- Evaluation of Low Back Pain in Adults - UpToDateDocument25 pagesEvaluation of Low Back Pain in Adults - UpToDateJeissonPargaSalasNo ratings yet
- Screening For Medical Problems in Patients With Upper Extremity Signs and SymptomsDocument23 pagesScreening For Medical Problems in Patients With Upper Extremity Signs and SymptomskerolosNo ratings yet
- Physiotherapy Management of Neck Pain: Arianne P VerhagenDocument7 pagesPhysiotherapy Management of Neck Pain: Arianne P VerhagenHari25885No ratings yet
- Jurnal Gadar Internasional IDocument9 pagesJurnal Gadar Internasional IAlfanIndraNo ratings yet
- An Introduction To The Use of Epidemiologic Research Methods in Dairy ScienceDocument8 pagesAn Introduction To The Use of Epidemiologic Research Methods in Dairy ScienceAndre LanzerNo ratings yet
- Clinical Diagnosis of Endometriosis: A Call To ActionDocument12 pagesClinical Diagnosis of Endometriosis: A Call To ActionEvan DionesiaNo ratings yet
- Delirium in The Geriatric Patient: Risk Factors For DeliriumDocument5 pagesDelirium in The Geriatric Patient: Risk Factors For DeliriumDenyNo ratings yet
- D0005RDocument13 pagesD0005RGleycer Adela Rodríguez TorrealvaNo ratings yet
- Crp5 k3 Prog PceDocument33 pagesCrp5 k3 Prog PceAde IndrawanNo ratings yet
- My Approach To Interstitial Lung Disease Usingclinical, Radiological and Histopathological PatternsDocument15 pagesMy Approach To Interstitial Lung Disease Usingclinical, Radiological and Histopathological PatternsMarcelle FreireNo ratings yet
- Chest Pain EvaluationDocument23 pagesChest Pain Evaluationhjuarez1102No ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet
- Introduction To EpidemiologyDocument9 pagesIntroduction To EpidemiologythenalynnloyolaNo ratings yet
- A Study of Plain X-Ray Vs USG Abdomen in Acute Abdomen CasesDocument3 pagesA Study of Plain X-Ray Vs USG Abdomen in Acute Abdomen CasessumanNo ratings yet
- Evan's SyndromeDocument94 pagesEvan's SyndromeKristine Joy Vivero BillonesNo ratings yet
- Common Terminology Criteria For Adverse Events Following Chemotherapy or Biological Antineoplastic Therapy in Dogs and Cats. VCOG. 2011Document30 pagesCommon Terminology Criteria For Adverse Events Following Chemotherapy or Biological Antineoplastic Therapy in Dogs and Cats. VCOG. 2011Mario GonzálezNo ratings yet
- Compartir Geri OncoDocument4 pagesCompartir Geri OncoHenrikNo ratings yet
- Wisbey 1983Document3 pagesWisbey 1983Auliana FENo ratings yet
- Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsDocument34 pagesBrief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsCarlos CuadrosNo ratings yet
- Health Services and Outcomes ResearchDocument7 pagesHealth Services and Outcomes ResearchRodrigoSachiFreitasNo ratings yet
- Advances in The Diagnosis and Management of Neck PainDocument19 pagesAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezNo ratings yet
- Delirium in The Elderly: A ReviewDocument20 pagesDelirium in The Elderly: A ReviewsaudahNo ratings yet
- DickDocument6 pagesDickNadirah Abd HamidNo ratings yet
- Falls NejmDocument8 pagesFalls NejmBrijesh Jani CPC JamnagarNo ratings yet
- M. Yusof (Dawood, M.D., M.MED. M.R.C.O.G.: University of College of Chicago, LlinoisDocument9 pagesM. Yusof (Dawood, M.D., M.MED. M.R.C.O.G.: University of College of Chicago, LlinoisS MpNo ratings yet
- Step2 2002 Answers PDFDocument87 pagesStep2 2002 Answers PDFZioFalzNo ratings yet
- Graves 2007Document10 pagesGraves 2007Christine HandayaniNo ratings yet
- DialoguesClinNeurosci 13 101Document8 pagesDialoguesClinNeurosci 13 101Fira KhasanahNo ratings yet
- Case Series - Acute Coronary SyndromeDocument18 pagesCase Series - Acute Coronary SyndromenikNo ratings yet
- Cervical Facet PainDocument11 pagesCervical Facet PainthiagoNo ratings yet
- Care of The Critically Ill Patient: Jeffrey J. Presneill and John F. CadeDocument5 pagesCare of The Critically Ill Patient: Jeffrey J. Presneill and John F. CadeDataeka InfoNo ratings yet
- Dor LombarDocument27 pagesDor LombarLeonardoCampanelliNo ratings yet
- DiverticularDiseaseoftheColon PDFDocument12 pagesDiverticularDiseaseoftheColon PDFAdrian MucileanuNo ratings yet
- CIRSG Manual EDocument30 pagesCIRSG Manual EBryanJermyHendrikNo ratings yet
- Medical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellDocument7 pagesMedical Management of Acute Severe Anorexia Nervosa: Amy Norrington, Ruth Stanley, Michael Tremlett, Ginny BirrellMarioNo ratings yet
- European J of Heart Fail - 2016 - Vid NDocument7 pagesEuropean J of Heart Fail - 2016 - Vid NfelipeNo ratings yet
- כאב בטןDocument5 pagesכאב בטןddNo ratings yet
- Delirium in Hospitalized Older AdultsDocument11 pagesDelirium in Hospitalized Older AdultsNavodith FernandoNo ratings yet
- S C R S C: Ymptom Lusters Elated To Pecific AncersDocument6 pagesS C R S C: Ymptom Lusters Elated To Pecific AncersDip Ayan MNo ratings yet
- Úlceras Por EstrésDocument5 pagesÚlceras Por Estrésanalisador analsiadorNo ratings yet
- Advances in The Diagnosis & Management of Neck Pain - Article.Document19 pagesAdvances in The Diagnosis & Management of Neck Pain - Article.salmankhan09215No ratings yet
- Red Flags For Serious Disease Causing LBP 10.07Document6 pagesRed Flags For Serious Disease Causing LBP 10.07Stefanie LeowardiNo ratings yet
- Case Presentat ION: Group No 2 Subgroup 2 Sec C Garge Shrikant Harish 33 Gunasekaran Janani 37 Kurpat Musthabeen 49Document27 pagesCase Presentat ION: Group No 2 Subgroup 2 Sec C Garge Shrikant Harish 33 Gunasekaran Janani 37 Kurpat Musthabeen 49Zedd ZorïNo ratings yet
- Respiratory Disorders: Dr. Fajar Wahyu PribadiDocument66 pagesRespiratory Disorders: Dr. Fajar Wahyu PribadiwinarsohNo ratings yet
- See Radiology Like Never Before.: KDR AU-DDR SystemDocument6 pagesSee Radiology Like Never Before.: KDR AU-DDR SystemFanof EcdNo ratings yet
- Topic: Asthma and Copd: Internal Medicine IiDocument8 pagesTopic: Asthma and Copd: Internal Medicine IicarlosNo ratings yet
- Full Download Test Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane Klein PDF Full ChapterDocument36 pagesFull Download Test Bank For Pathophysiology Concepts of Human Disease 1st Edition Matthew Sorenson Lauretta Quinn Diane Klein PDF Full Chapterpicheywitlingaip34100% (20)
- Part One - (Questions 1 - 10) : 1 Test 7Document7 pagesPart One - (Questions 1 - 10) : 1 Test 7SuliemanNo ratings yet
- Understand Congestive Heart FailureDocument5 pagesUnderstand Congestive Heart FailureOanh HoangNo ratings yet
- 2015 - Palliative Care in OncologyDocument302 pages2015 - Palliative Care in OncologyJuliaSandu100% (3)
- Asthma - Child - Discharge: When You're in The HospitalDocument15 pagesAsthma - Child - Discharge: When You're in The HospitalJu Lie AnnNo ratings yet
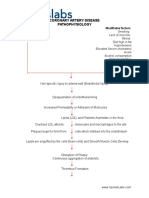
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Ob Database DXRDocument9 pagesOb Database DXRNMD LIFESAVERNo ratings yet
- Clinical Scenarios (2) 1 1Document6 pagesClinical Scenarios (2) 1 1Marzio FagioliNo ratings yet
- Geron-Ppt - 20231206 131738 0000Document29 pagesGeron-Ppt - 20231206 131738 0000Potato TomatoNo ratings yet
- The Lessons of Quantec Recommendations For Reporting and Gathering Data On Dose-Volume Dependencies of Treatment OutcomeDocument6 pagesThe Lessons of Quantec Recommendations For Reporting and Gathering Data On Dose-Volume Dependencies of Treatment OutcomeCarina Isabel Bento Marques CoelhoNo ratings yet
- Case Presentation Respiratory SystemDocument23 pagesCase Presentation Respiratory SystemShubhamNo ratings yet
- Latihan Abbreviation 2Document2 pagesLatihan Abbreviation 2Sherly AmeliaNo ratings yet
- Urografin Data SheetDocument17 pagesUrografin Data SheetYuanita PurnamiNo ratings yet
- Drill #1 With RationaleDocument12 pagesDrill #1 With RationaleRellie CastroNo ratings yet
- PALS Provider ManualDocument51 pagesPALS Provider Manualdanix manaliliNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2021 PEDIATRICSDocument112 pagesInformation MSQ KROK 2 Medicine 2007 2021 PEDIATRICSReshma Shaji PnsNo ratings yet
- Pleural Effusion Secondary To Community Acquired Pneumonia PathophysiologyDocument5 pagesPleural Effusion Secondary To Community Acquired Pneumonia PathophysiologySteffiNo ratings yet
- NCP 1Document5 pagesNCP 1Charm TanyaNo ratings yet
- Nursing Diagnosis For AsthmaDocument6 pagesNursing Diagnosis For AsthmaTINAIDA33% (3)
- Neonatal Respiratory DistressDocument54 pagesNeonatal Respiratory DistressMohamad Saleh100% (1)
- Pneumonia Concept MapDocument11 pagesPneumonia Concept Mapiz11100% (3)
- NCLEX Test Questions With RationaleDocument46 pagesNCLEX Test Questions With Rationaletetmetrangmail.com tet101486No ratings yet
- Presentasi Radiologi Edema ParuDocument19 pagesPresentasi Radiologi Edema ParuFia100% (1)
- Heart Medicines HomeopathicDocument6 pagesHeart Medicines Homeopathicwaseem_karachiNo ratings yet
- Shadow Health Cognition SubjectiveDocument7 pagesShadow Health Cognition Subjectiveqwivy.comNo ratings yet
- Patient Safety and Patient Assessment in Pre-Hospital Care: A Study ProtocolDocument7 pagesPatient Safety and Patient Assessment in Pre-Hospital Care: A Study ProtocolDeby KurniawanNo ratings yet