You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pulmonary Function Test (PFT)Document24 pagesPulmonary Function Test (PFT)hm3398No ratings yet
- Quill Love LettersDocument8 pagesQuill Love LettersDiego AndradeNo ratings yet
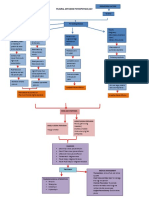
- Pleurl Effusion Pathophysiology DiagramDocument2 pagesPleurl Effusion Pathophysiology DiagramAkiraMamo67% (3)
- FU - The - Freeform - Universal - RPG - (Classic - Rules) 2Document24 pagesFU - The - Freeform - Universal - RPG - (Classic - Rules) 2Diego AndradeNo ratings yet
- Micro Chapbook RPG: Room Chart (D6)Document2 pagesMicro Chapbook RPG: Room Chart (D6)Diego Andrade0% (1)
- Pulmonary DisordersDocument53 pagesPulmonary DisordersAhmad Makhlouf100% (1)
- RESPI QuestionDocument14 pagesRESPI QuestionCarmela Marie Eriguel CuetoNo ratings yet
- Scientific Book Jicccim 2018Document171 pagesScientific Book Jicccim 2018ngwinda90No ratings yet
- Pocket Fantasy RPG Ver. 3.6Document4 pagesPocket Fantasy RPG Ver. 3.6Diego AndradeNo ratings yet
- Mechanical VentilatorDocument9 pagesMechanical VentilatorAnusha Verghese100% (2)
- Modes of Mechanical VentilationDocument34 pagesModes of Mechanical Ventilationsbraj86100% (1)
- NCP Bronchila Ashma Dra.Document3 pagesNCP Bronchila Ashma Dra.ЯicaЯdo BautistaNo ratings yet
- LAMU Term 1B IMED Written ExamDocument12 pagesLAMU Term 1B IMED Written ExamSecret AgentNo ratings yet
- A Lonely Knave Solo Roleplay (Knave)Document2 pagesA Lonely Knave Solo Roleplay (Knave)Diego Andrade0% (1)
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Non Invasive Ventilation and Weaning PDFDocument748 pagesNon Invasive Ventilation and Weaning PDFAny Córdova100% (2)
- Tecme Neumovent Technical Manual 94Document94 pagesTecme Neumovent Technical Manual 94Marina Garza GaliciaNo ratings yet
- BTS Guidelines For The Management of Pleural Infection in ChildrenDocument21 pagesBTS Guidelines For The Management of Pleural Infection in ChildrenDiego AndradeNo ratings yet
- Randomised Trial of Intrapleural Urokinase in The Treatment of Childhood EmpyemaDocument5 pagesRandomised Trial of Intrapleural Urokinase in The Treatment of Childhood EmpyemaDiego AndradeNo ratings yet
- 839 1 FullDocument3 pages839 1 FullDiego AndradeNo ratings yet
- Thoracic EmpyemaDocument3 pagesThoracic EmpyemaDiego AndradeNo ratings yet
- RCCM 200601-027ocDocument7 pagesRCCM 200601-027ocDiego AndradeNo ratings yet
- Camargos 2015Document6 pagesCamargos 2015Diego AndradeNo ratings yet
- CRGE Conjectural Roleplaying GM EmulatorDocument32 pagesCRGE Conjectural Roleplaying GM EmulatorDiego AndradeNo ratings yet
- Dodi Daftar PustakaDocument3 pagesDodi Daftar PustakaToni PinemNo ratings yet
- Persistent Cough in ChildrenDocument6 pagesPersistent Cough in Childrenyujin KimNo ratings yet
- HemothoraxDocument27 pagesHemothoraxShreyasi AnkushNo ratings yet
- BiPAP A40 - BrochureDocument2 pagesBiPAP A40 - BrochureDonny AndiNo ratings yet
- # Davidson - Review # Respiratory - MedicineDocument18 pages# Davidson - Review # Respiratory - Medicineemtiaz zamanNo ratings yet
- Pocket Guide For Asthma Management and PreventionDocument33 pagesPocket Guide For Asthma Management and PreventionRiaNo ratings yet
- Catalog - Intra Catheters - SemnatDocument4 pagesCatalog - Intra Catheters - SemnatFatima VessaliusNo ratings yet
- Reflection Respiratory SystemDocument4 pagesReflection Respiratory SystemAin Sufiza0% (1)
- Thoracic Emergency Trauma QuestionnairesDocument7 pagesThoracic Emergency Trauma QuestionnairesMeliza BancolitaNo ratings yet
- Assessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesDocument15 pagesAssessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesJhosita Flora LarocoNo ratings yet
- History and Physical Exam For COPDDocument10 pagesHistory and Physical Exam For COPDCathy GuerreroNo ratings yet
- JSS MoUDocument88 pagesJSS MoUchetanhiremathNo ratings yet
- Normal and Abnormal Findings of Thorax and LungsDocument3 pagesNormal and Abnormal Findings of Thorax and LungsOtherin Ojibwa TejanoNo ratings yet
- E60a4042 ME2512 Medicine 1 Respiratory 2023-2024Document39 pagesE60a4042 ME2512 Medicine 1 Respiratory 2023-2024Iona PatrickNo ratings yet
- Jarvis Chapter 18 Study GuideDocument5 pagesJarvis Chapter 18 Study GuideEmily Cheng100% (2)
- No. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderDocument6 pagesNo. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderFatimah AzzahraNo ratings yet
- Weaning ProtocolDocument6 pagesWeaning ProtocolerwanNo ratings yet
- 2006 129 1344-1348 Christopher E. Brightling: Clinical Applications of Induced SputumDocument7 pages2006 129 1344-1348 Christopher E. Brightling: Clinical Applications of Induced Sputumjoal510No ratings yet