You might also like
- Structure and Function of The Endocrine and Metabolic SystemDocument21 pagesStructure and Function of The Endocrine and Metabolic Systemcoy008No ratings yet
- Endocrine System Pathology and Nursing ManagementDocument30 pagesEndocrine System Pathology and Nursing Managementseries recapNo ratings yet
- Hyperparathyroidism and HypoparathyroidismDocument44 pagesHyperparathyroidism and Hypoparathyroidismshweta singhNo ratings yet
- Major Hormone Glands and Their FunctionsDocument5 pagesMajor Hormone Glands and Their FunctionsSTEFFI GABRIELLE GOLEZNo ratings yet
- A Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesFrom EverandA Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesNo ratings yet
- Endocrine: Common Lab Tests For Endocrine and Hormonal DisordersDocument19 pagesEndocrine: Common Lab Tests For Endocrine and Hormonal DisordersPhilip SimanganNo ratings yet
- Pharmacology Test 3 ReviewDocument6 pagesPharmacology Test 3 ReviewNatalia BortellNo ratings yet
- Endocrine Group 1Document25 pagesEndocrine Group 1Shermine Keith DoctoleroNo ratings yet
- Diseases of The Adrenal GlandsDocument27 pagesDiseases of The Adrenal GlandsPurnima ChoudhuryNo ratings yet
- Module 3-Specimen Collection and ProcessingDocument10 pagesModule 3-Specimen Collection and ProcessingAllyah Ross DuqueNo ratings yet
- Hyperuricemia Case DiscussionDocument7 pagesHyperuricemia Case DiscussionVineth MartinNo ratings yet
- Endocrine Focus PointsDocument10 pagesEndocrine Focus PointsHayden ShulerNo ratings yet
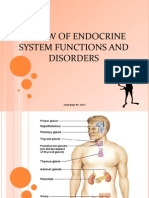
- Review of Endocrine System Functions and Disorders: Arnel Ipapo RN, MANDocument51 pagesReview of Endocrine System Functions and Disorders: Arnel Ipapo RN, MANcha_cha_magistradoNo ratings yet
- Hormonal regulation study guide for NURS 320 Exam 2Document15 pagesHormonal regulation study guide for NURS 320 Exam 2Anthony Del RioNo ratings yet
- Endocrine NursingDocument8 pagesEndocrine NursingBunny Bonny100% (5)
- Endocrine DisordersDocument16 pagesEndocrine DisordersEiffel AnchetaNo ratings yet
- Oncologic Emergencies Classification and TreatmentDocument41 pagesOncologic Emergencies Classification and Treatmentomad pendaftaranPPDS100% (2)
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Parathyroid Glands: Anatomy, Function and DisordersDocument28 pagesParathyroid Glands: Anatomy, Function and DisordersOmar Alruwaili100% (1)
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- Pathology of Adrenal Glands.Document41 pagesPathology of Adrenal Glands.Sukma Eka PratiwiNo ratings yet
- Cushing's Syndrome: Diagnosis, Treatment and Nursing CareDocument2 pagesCushing's Syndrome: Diagnosis, Treatment and Nursing CareCourtney HammonsNo ratings yet
- Endocrine RevisonDocument21 pagesEndocrine Revisonalistair.james.clarkeNo ratings yet
- Addison DiseaseDocument23 pagesAddison DiseaseKompari EvansNo ratings yet
- Endocrine Disorders and DrugsDocument149 pagesEndocrine Disorders and DrugsJaypee Fabros Edra100% (1)
- Definition - Cushing's Syndrome Is The Combination of Symptoms and SignsDocument4 pagesDefinition - Cushing's Syndrome Is The Combination of Symptoms and SignsSuhas IngaleNo ratings yet
- Electrolytes Imbalances: Prepared By: Mr. Charlie C. Falguera, RNDocument35 pagesElectrolytes Imbalances: Prepared By: Mr. Charlie C. Falguera, RNJarvin RenomeronNo ratings yet
- Med/Surg Nursing: Endocrine System-2009Document127 pagesMed/Surg Nursing: Endocrine System-2009arbyjamesNo ratings yet
- Parathyroid Glands: Hyperparathyroidism and HypoparathyroidismDocument3 pagesParathyroid Glands: Hyperparathyroidism and HypoparathyroidismStrong Woman Bong SoonNo ratings yet
- Disorders of The Adrenal GlandsDocument9 pagesDisorders of The Adrenal Glandsmoon businessNo ratings yet
- Cushing Syndrome: Clinical ManifestationsDocument4 pagesCushing Syndrome: Clinical ManifestationsMikko Anthony Pingol AlarconNo ratings yet
- Medical Surgical Nursing 1Document333 pagesMedical Surgical Nursing 1Divine BitancurNo ratings yet
- Endocrine Study GuideDocument4 pagesEndocrine Study GuideNursingSchoolNotes100% (1)
- Addison's DiseaseDocument27 pagesAddison's DiseaseismaylkympotNo ratings yet
- Cushing's SyndromeDocument68 pagesCushing's SyndromeKaye De Guzman, BSN - Level 3ANo ratings yet
- HyperparathyroidismDocument5 pagesHyperparathyroidismLyra Lorca75% (12)
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- Disorders of Adrenal GlandsDocument48 pagesDisorders of Adrenal GlandsCharlz ZipaganNo ratings yet
- KMB II Sistem Endokrin PT IIDocument68 pagesKMB II Sistem Endokrin PT IIAngel ChrisNo ratings yet
- Nursing Care of Client With Endocrine DisorderDocument93 pagesNursing Care of Client With Endocrine DisorderApril_Anne_Vel_343No ratings yet
- Adrenal Disorder 1Document32 pagesAdrenal Disorder 1vanthygNo ratings yet
- Endocrine SystemDocument8 pagesEndocrine Systemtheglobalnursing80% (5)
- Pheo Esrd and NeonateDocument45 pagesPheo Esrd and NeonateLea TanNo ratings yet
- ENDOCRINEDocument5 pagesENDOCRINERizMarie100% (3)
- Sheep and goat gastrointestinal and respiratory diseasesDocument5 pagesSheep and goat gastrointestinal and respiratory diseasesJessica Elizabeth JosephNo ratings yet
- Disorders of The Adrenal Gland LectureDocument36 pagesDisorders of The Adrenal Gland LectureBars DenskieNo ratings yet
- Endocrine Reviews UndanaDocument132 pagesEndocrine Reviews UndanaAndi Suchy Qumala SarieNo ratings yet
- Adrenal Glands: Adrenal Cortex Adrenal MedullaDocument66 pagesAdrenal Glands: Adrenal Cortex Adrenal MedullaRinto NugrohoNo ratings yet
- Renal CalculiDocument28 pagesRenal Calculihailleyann33% (3)
- EndocrinologyDocument34 pagesEndocrinologymiyuchix100% (2)
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamDocument36 pagesDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaNo ratings yet
- Endocrine SystemDocument25 pagesEndocrine Systemangel_maui100% (13)
- Adrenal Gland Disorders ExplainedDocument73 pagesAdrenal Gland Disorders ExplainedReunita ConstantiaNo ratings yet
- Anaesthesia in Parathyroid Gland Disorders and Calcium MetabolismDocument25 pagesAnaesthesia in Parathyroid Gland Disorders and Calcium MetabolismAshiyan IrfanNo ratings yet
- Adrenal and Thyroid Gland Disorders ExplainedDocument39 pagesAdrenal and Thyroid Gland Disorders ExplainedJanine Dela CruzNo ratings yet
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- Pharma Medications ListDocument35 pagesPharma Medications ListCalvin Keith YadaoNo ratings yet
- ESSAY PediaDocument2 pagesESSAY PediaCalvin Keith YadaoNo ratings yet
- Hand Scrub ProcedureDocument1 pageHand Scrub ProcedureCalvin Keith YadaoNo ratings yet
- Rotc Doc1Document15 pagesRotc Doc1Calvin Keith YadaoNo ratings yet
- Therapeutic NurseDocument4 pagesTherapeutic NurseCalvin Keith YadaoNo ratings yet
- ESSAY PediaDocument2 pagesESSAY PediaCalvin Keith YadaoNo ratings yet
- HypermagnesemiaDocument2 pagesHypermagnesemiaCalvin Keith YadaoNo ratings yet
- Ds Heparin SodiumDocument3 pagesDs Heparin SodiumCalvin Keith YadaoNo ratings yet
- Drug Education Chapter Provides InsightDocument13 pagesDrug Education Chapter Provides InsightCalvin Keith YadaoNo ratings yet
- Outcome Goal: Outcome Goal: byDocument2 pagesOutcome Goal: Outcome Goal: byCalvin Keith YadaoNo ratings yet
- Albuterol DsDocument2 pagesAlbuterol DsCalvin Keith YadaoNo ratings yet
- Hormone Health Newsletter Provides Tips for Pregnancy, Weight LossDocument10 pagesHormone Health Newsletter Provides Tips for Pregnancy, Weight LossBrian CoxNo ratings yet
- Laboratory Tests for Evaluating Adrenal InsufficiencyDocument9 pagesLaboratory Tests for Evaluating Adrenal InsufficiencyConciliatorNo ratings yet
- Adrenal Hormone 2018 PDFDocument66 pagesAdrenal Hormone 2018 PDFrosyidafiaNo ratings yet
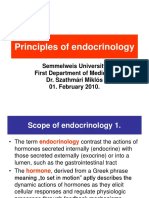
- Principles of endocrinology scope and functionsDocument25 pagesPrinciples of endocrinology scope and functionsRyan James Lorenzo MiguelNo ratings yet
- 2021-The Biology of Burnout Causes and ConsequencesDocument14 pages2021-The Biology of Burnout Causes and Consequencesxi LuNo ratings yet
- Humans evolved to thrive on restricted dietsDocument8 pagesHumans evolved to thrive on restricted dietsaman singhNo ratings yet
- Pyrroluria HPU-Questionnaire - Vragenlijst ENGLISH - WWW - Hputest.nl EnglishDocument26 pagesPyrroluria HPU-Questionnaire - Vragenlijst ENGLISH - WWW - Hputest.nl EnglishaxyzaaaNo ratings yet
- Cortisol and Belly Fat Part 2Document5 pagesCortisol and Belly Fat Part 2PaleoDieting100% (2)
- (English) How Stress Affects Your Brain - Madhumita Murgia (DownSub - Com)Document4 pages(English) How Stress Affects Your Brain - Madhumita Murgia (DownSub - Com)FE HonorNo ratings yet
- Decalcifiying Pineal GlandDocument8 pagesDecalcifiying Pineal Glandsonden_291% (11)
- Basics in Clinical Nutrition: Carbohydrate Metabolism: Luc TappyDocument4 pagesBasics in Clinical Nutrition: Carbohydrate Metabolism: Luc Tappymarliana100% (1)
- X traordinary4XMassWorkout PDFDocument51 pagesX traordinary4XMassWorkout PDFAnthony Davis100% (4)
- Review Tricaine Methane-Sulfonate (MS-222) Application in Fish AnaesthesiaDocument12 pagesReview Tricaine Methane-Sulfonate (MS-222) Application in Fish AnaesthesiaGuilherme Vasconcelos VasconcelosNo ratings yet
- Mousab Kibreet Notes of Internal Medicine 2ed EditionDocument253 pagesMousab Kibreet Notes of Internal Medicine 2ed EditionAbdulltif AliNo ratings yet
- Yoga Journal USA - Your 6-Week Yoga Guide To Build Strength 2017 PDFDocument118 pagesYoga Journal USA - Your 6-Week Yoga Guide To Build Strength 2017 PDFthesolomon100% (2)
- The Beacon EpaperDocument26 pagesThe Beacon EpaperCatawba SecurityNo ratings yet
- Holistic Healthcare For Transgender and Gender Variant Folks - Dori MidnightDocument17 pagesHolistic Healthcare For Transgender and Gender Variant Folks - Dori Midnightpille83100% (1)
- Super Longevity mp3 InstructionsDocument3 pagesSuper Longevity mp3 InstructionsjulioNo ratings yet
- Chapter 18 Endocrine SystemDocument40 pagesChapter 18 Endocrine SystemlolasparkleNo ratings yet
- Disorders of AdrenalsDocument8 pagesDisorders of AdrenalsM.PRASAD NAIDUNo ratings yet
- You Are the Placebo - How to Harness Your Innate Healing PowerDocument2 pagesYou Are the Placebo - How to Harness Your Innate Healing PowerManalaniLinh75% (4)
- Korte 2005Document36 pagesKorte 2005CellaNo ratings yet
- MCQ Questions End of Module EndocrineDocument9 pagesMCQ Questions End of Module EndocrineAlif Akmal100% (2)
- Adrenal CrisisDocument4 pagesAdrenal CrisisRichie Marie BajaNo ratings yet
- Assignment of Adrenal CortexDocument12 pagesAssignment of Adrenal CortexWania AliNo ratings yet
- Government SideDocument2 pagesGovernment SideDonna Jayne AlianzaNo ratings yet
- CHROUSOS, George 2009 - Stress and Disorders of The Stress SystemDocument8 pagesCHROUSOS, George 2009 - Stress and Disorders of The Stress SystemRafael MagalhãesNo ratings yet
- Mike Mahler - Live Life Aggressively! What Self-Help Gurus Should Be Telling YouDocument263 pagesMike Mahler - Live Life Aggressively! What Self-Help Gurus Should Be Telling Youbobsyaruncle4814100% (5)
- Download Best Of Five Mcqs For The Endocrinology And Diabetes Sce Atul Kalhan full chapterDocument67 pagesDownload Best Of Five Mcqs For The Endocrinology And Diabetes Sce Atul Kalhan full chapterdeanna.haire453100% (4)
- CAH Exploration: Theoretical Aspects and Daily Life IntegrationDocument17 pagesCAH Exploration: Theoretical Aspects and Daily Life IntegrationInani Nabila LahuriNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)