You might also like
- And Abliat Vrratti.: Noitur &Document12 pagesAnd Abliat Vrratti.: Noitur &luis titoNo ratings yet
- Legal Evolution and Systems in IndiaDocument28 pagesLegal Evolution and Systems in Indiaakash nakkiranNo ratings yet
- HSC ENGLISH REDUCED SYLLABUS REVISION NOTESDocument72 pagesHSC ENGLISH REDUCED SYLLABUS REVISION NOTESMohamed Jamil IrfanNo ratings yet
- Philo - Chapter 5 - ls1-5Document5 pagesPhilo - Chapter 5 - ls1-5Precious Gem PortugalNo ratings yet
- Autistic Females in The United KingdomDocument12 pagesAutistic Females in The United Kingdomapi-659812277No ratings yet
- Scour Behaviour and Scour Protection For MonopileDocument15 pagesScour Behaviour and Scour Protection For MonopileWilliam HoNo ratings yet
- The Mystery of The Mystics and A Scientific Vision Uncovering A New RealityDocument2 pagesThe Mystery of The Mystics and A Scientific Vision Uncovering A New RealityChirag ChhabriaNo ratings yet
- Free Health Check-Up Camps and Medicine DistributionDocument13 pagesFree Health Check-Up Camps and Medicine DistributionIRDP INDIANo ratings yet
- Santiago: Customer Service SCLDocument9 pagesSantiago: Customer Service SCLArdXkillerNo ratings yet
- Final - IT8761 Security Lab ManualDocument55 pagesFinal - IT8761 Security Lab ManualShiek TiwariNo ratings yet
- Senate Bill 2247Document4 pagesSenate Bill 2247inforumdocsNo ratings yet
- PelangiDocument13 pagesPelangiFAHMA IQBALNo ratings yet
- 52 MANE-003 Comparative Ethnography Block-7 Gender and SexualitiesDocument41 pages52 MANE-003 Comparative Ethnography Block-7 Gender and Sexualitiestwinkle0% (1)
- Biology Project File 12thDocument22 pagesBiology Project File 12thNaveen SharmaNo ratings yet
- 4D PRINTING OF NITINOL APPLICATIONSDocument7 pages4D PRINTING OF NITINOL APPLICATIONSAbid YusufNo ratings yet
- Curriculum Vitae: Zaw Zaw Project Engineer (Power)Document6 pagesCurriculum Vitae: Zaw Zaw Project Engineer (Power)Htet WaiNo ratings yet
- Pro Ramming Massesl CumiramDocument3 pagesPro Ramming Massesl Cumiramashudeva12No ratings yet
- Guide to Writing Effective Essays for English Proficiency TestsDocument25 pagesGuide to Writing Effective Essays for English Proficiency Testslê myNo ratings yet
- NGA Standard Defines DoD WGS 84Document207 pagesNGA Standard Defines DoD WGS 84mmNo ratings yet
- RACP Assessment and Selection: Developing Extended Matching Questions (EMQsDocument9 pagesRACP Assessment and Selection: Developing Extended Matching Questions (EMQsRuth MungaiNo ratings yet
- Bài tập tự động hóa sản xuất - 0001-0001Document1 pageBài tập tự động hóa sản xuất - 0001-0001Minh NhậtNo ratings yet
- 00 Registration - Form VER 2.0Document4 pages00 Registration - Form VER 2.0Dr.Shrikant DwivediNo ratings yet
- RAGHU Final ProjectDocument50 pagesRAGHU Final ProjectPrakashNo ratings yet
- Application To RevokeDocument6 pagesApplication To RevokeOKCFOXNo ratings yet
- LT Marine Crew ApplicationDocument4 pagesLT Marine Crew ApplicationEirvin JamesNo ratings yet
- Pry 6 Phe 3RD TermDocument31 pagesPry 6 Phe 3RD Termsamuel joshuaNo ratings yet
- Florence Nightingale Theory: She Emphasizes Five Essential Point in Securing Health of HouseDocument2 pagesFlorence Nightingale Theory: She Emphasizes Five Essential Point in Securing Health of HouseAkshata BansodeNo ratings yet
- Texas LS Notes 19-20Document2 pagesTexas LS Notes 19-20Jesus del CampoNo ratings yet
- Icmp Placement Brochure 22-24Document13 pagesIcmp Placement Brochure 22-24Siva VanjariNo ratings yet
- Analysis of The Advantages of The M1 CPU and Its Impact On The Future Development of AppleDocument4 pagesAnalysis of The Advantages of The M1 CPU and Its Impact On The Future Development of ApplepaolabioNo ratings yet
- IOT Project POSTERDocument1 pageIOT Project POSTERFemilNo ratings yet
- Is-4128 Fireman's Leather BootsDocument14 pagesIs-4128 Fireman's Leather BootsCharls James100% (1)
- Marathon NotesDocument341 pagesMarathon NotesLokesh Agarwalla100% (1)
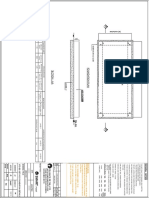
- Foundation plan and details for commercial buildingDocument1 pageFoundation plan and details for commercial buildingajay kumarNo ratings yet
- S Pater 2020Document16 pagesS Pater 2020jujofegiNo ratings yet
- DANC254 Example 5Document3 pagesDANC254 Example 5Bambang HariyantoNo ratings yet
- TU PHD Booklet2021300Document66 pagesTU PHD Booklet2021300achyutNo ratings yet
- Lgu - Local Monitoring Forms 1 5Document6 pagesLgu - Local Monitoring Forms 1 5Jenefer GarciaNo ratings yet
- Disney PatentDocument12 pagesDisney PatentCharles GrossNo ratings yet
- Smart Drive Two Wheeler InsuranceDocument2 pagesSmart Drive Two Wheeler InsuranceAaditya raj SuryaNo ratings yet
- ISA 3.0 E-Learning Assessment TestDocument20 pagesISA 3.0 E-Learning Assessment TestCAAniketGangwalNo ratings yet
- Assignment 1Document2 pagesAssignment 110aet cadNo ratings yet
- Productive Resources Lesson PlanDocument3 pagesProductive Resources Lesson PlanLakira WoodsNo ratings yet
- IKM Online Assessment ResultDocument1 pageIKM Online Assessment ResultpattabhikvNo ratings yet
- Mixtures and SeparationDocument43 pagesMixtures and SeparationTrudy- Ann CaineNo ratings yet
- YASHU Final Technical Seminar ReportDocument23 pagesYASHU Final Technical Seminar Reportyashwanth vNo ratings yet
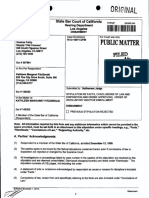
- Kathleen Margaret Fitzgerald 145252 California 16-O-16571-3Document82 pagesKathleen Margaret Fitzgerald 145252 California 16-O-16571-3juanguzman5No ratings yet
- Fall Sports Preview (2022)Document24 pagesFall Sports Preview (2022)Watertown Daily TimesNo ratings yet
- AME 204 Spring 2012 Midterm Exam I SolutionDocument6 pagesAME 204 Spring 2012 Midterm Exam I SolutionJack ZhaoNo ratings yet
- Grade 3 Fixed ModulDocument98 pagesGrade 3 Fixed ModulIndra Yusuf PurnamaNo ratings yet
- From Gene Banks To FarmersDocument58 pagesFrom Gene Banks To FarmersPuran pataNo ratings yet
- #Rxinott.: Sabbath RaidDocument12 pages#Rxinott.: Sabbath Raidluis titoNo ratings yet
- D6587-12e1 Standard Test Method For Yarn Number Using Automatic TesterDocument6 pagesD6587-12e1 Standard Test Method For Yarn Number Using Automatic TesterAswindana Ibnu SenaNo ratings yet
- The Legend of BananaDocument1 pageThe Legend of BananaMonina CarreonNo ratings yet
- AP Physics C Electricity and Magnetism Course at A GlanceDocument2 pagesAP Physics C Electricity and Magnetism Course at A GlanceJashanbir SinghNo ratings yet
- Add-On KYC Renewal Form: Recent Photo of The Add-On Cardholder (1) Recent Photo of The Add-On CardholderDocument1 pageAdd-On KYC Renewal Form: Recent Photo of The Add-On Cardholder (1) Recent Photo of The Add-On CardholderUday KrishnaNo ratings yet
- As 129959 Iv3-G500ca Iv3-G500ma Iv3-G600ca Im 96M17460 WW GB 2102 1Document2 pagesAs 129959 Iv3-G500ca Iv3-G500ma Iv3-G600ca Im 96M17460 WW GB 2102 1AfifNasirNo ratings yet
- Design, Construction, Modification, Maintenance and Decommissioning of Filling StationsDocument320 pagesDesign, Construction, Modification, Maintenance and Decommissioning of Filling StationsMaurizio BusuNo ratings yet
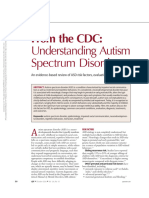
- From the CDC Understanding Autism Spectrum DisorderDocument8 pagesFrom the CDC Understanding Autism Spectrum DisorderEliza MedeirosNo ratings yet
- Habilidade de Vida Diaria No TEA de 2 A 22 Anos PDFDocument11 pagesHabilidade de Vida Diaria No TEA de 2 A 22 Anos PDF4nt0n jun10rNo ratings yet
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)
- Fee Structure 2023-2024Document10 pagesFee Structure 2023-2024Emmanuel NjogellahNo ratings yet
- (Jean Oliver and Alison Middleditch (Auth.) ) Funct (B-Ok - CC)Document332 pages(Jean Oliver and Alison Middleditch (Auth.) ) Funct (B-Ok - CC)Lorena BurdujocNo ratings yet
- IruvarDocument5 pagesIruvarKarthikeya KaredlaNo ratings yet
- Christopher Westra - Laws of Attraction PDFDocument3 pagesChristopher Westra - Laws of Attraction PDFZachary LeeNo ratings yet
- Ffective Riting Kills: Training & Discussion OnDocument37 pagesFfective Riting Kills: Training & Discussion OnKasi ReddyNo ratings yet
- NYC Chocolate Chip Cookies! - Jane's PatisserieDocument2 pagesNYC Chocolate Chip Cookies! - Jane's PatisserieCharmaine IlaoNo ratings yet
- DANGEL 4as LESSON PLANNINGDocument2 pagesDANGEL 4as LESSON PLANNINGCarlz BrianNo ratings yet
- How Can I Have Faith - Discussion GuideDocument6 pagesHow Can I Have Faith - Discussion GuideFrank Edwin VedamNo ratings yet
- 6.1.2 The Solar SystemDocument4 pages6.1.2 The Solar System205 NursyazliyanaNo ratings yet
- Sharp Sharp Cash Register Xe A207 Users Manual 284068Document1 pageSharp Sharp Cash Register Xe A207 Users Manual 284068Zeila CordeiroNo ratings yet
- Junguian PsychotherapyDocument194 pagesJunguian PsychotherapyRene Galvan Heim100% (13)
- Signals and Systems Analysis: NET 351 Instructor: Dr. Amer El-Khairy يريخلا &رماع .دDocument44 pagesSignals and Systems Analysis: NET 351 Instructor: Dr. Amer El-Khairy يريخلا &رماع .دمصعب جاسمNo ratings yet
- PRESSURE VESSEL Handbook - Eugene F. Megyesy 12th 2001Document501 pagesPRESSURE VESSEL Handbook - Eugene F. Megyesy 12th 2001vamcodong71% (7)
- Ruach Ha Kodesh or Holy Religious SpiritDocument10 pagesRuach Ha Kodesh or Holy Religious Spiritharsan100% (1)
- DP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDocument213 pagesDP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDaniel JuarezNo ratings yet
- ISO 13485 Version 2016 Requirements NotesDocument24 pagesISO 13485 Version 2016 Requirements Notesda_reaper_dasNo ratings yet
- Pizza Hut Final!Document15 pagesPizza Hut Final!Alisha ParabNo ratings yet
- Building Lean Supply ChainsDocument33 pagesBuilding Lean Supply ChainsJefri MustaphaNo ratings yet
- Keto Food List for BodybuildingDocument8 pagesKeto Food List for Bodybuildingharris81No ratings yet
- Development PlanningDocument15 pagesDevelopment PlanningSamuelNo ratings yet
- Template Project Approach QuestionnaireDocument1 pageTemplate Project Approach QuestionnaireSara AliNo ratings yet
- CBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and SaltsDocument11 pagesCBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and Saltsmilind dhamaniyaNo ratings yet
- Exam Unit 1 Out and About 1º BachilleratoDocument5 pagesExam Unit 1 Out and About 1º Bachilleratolisikratis1980No ratings yet
- IM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04Document7 pagesIM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04oliwia bujalskaNo ratings yet
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet
- Bridge Manual Retaining Walls - Section 3.62 Page 3.2-2Document1 pageBridge Manual Retaining Walls - Section 3.62 Page 3.2-2lomoscribdNo ratings yet
- Horizontal Projectile MotionDocument17 pagesHorizontal Projectile MotionMark BagamaspadNo ratings yet
- Accounting For Non Specialists Australian 7th Edition Atrill Test BankDocument26 pagesAccounting For Non Specialists Australian 7th Edition Atrill Test BankJessicaMitchelleokj100% (49)
- Guidelines SLCM BWDocument60 pagesGuidelines SLCM BWpnaarayanNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: Hidden Potential: The Science of Achieving Greater Things By Adam Grant: Key Takeaways, Summary and AnalysisFrom EverandSummary: Hidden Potential: The Science of Achieving Greater Things By Adam Grant: Key Takeaways, Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (15)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)